

Ultrasound findings in urogenital schistosomiasis: a pictorial essay
- PMID: 31494862
- PMCID: PMC7242546
- DOI: 10.1007/s40477-019-00405-1
Ultrasound findings in urogenital schistosomiasis: a pictorial essay
Abstract
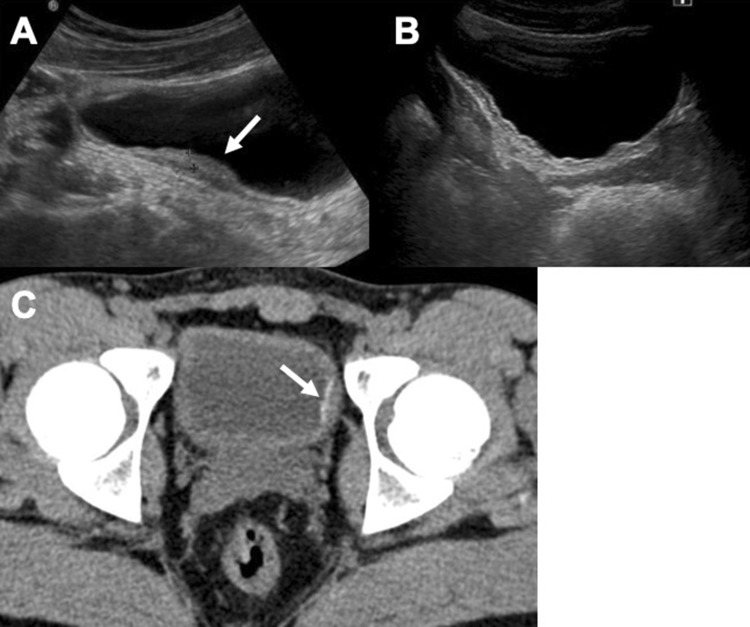
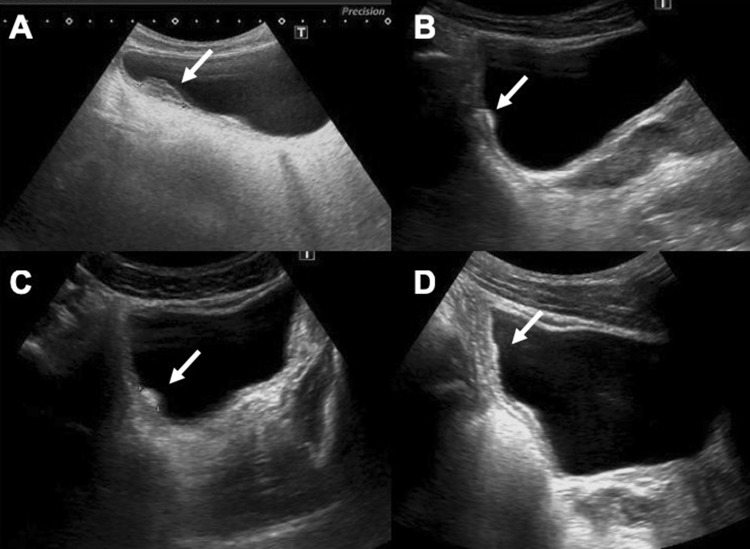
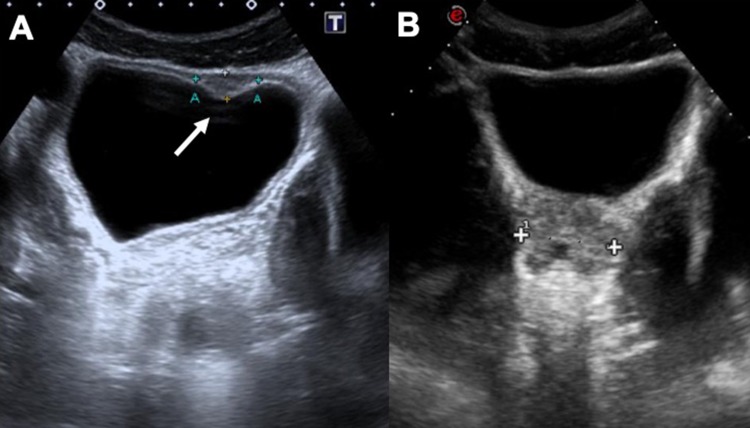
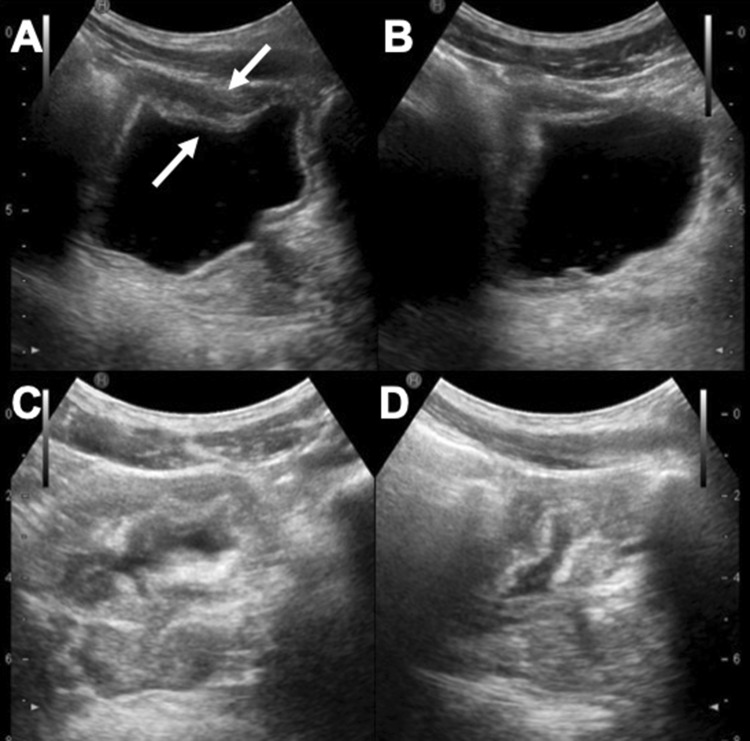
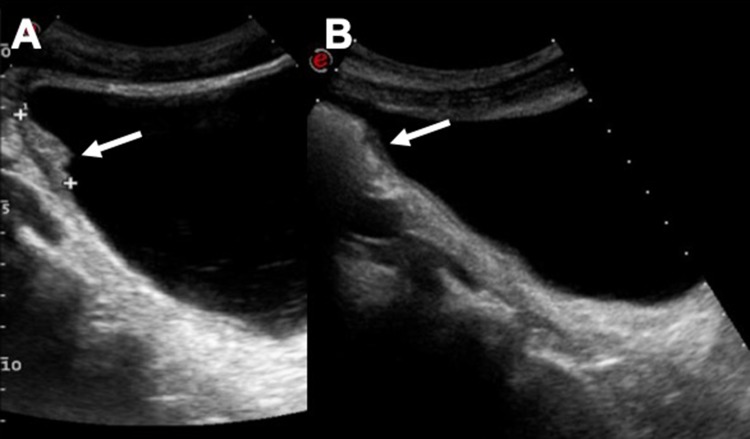
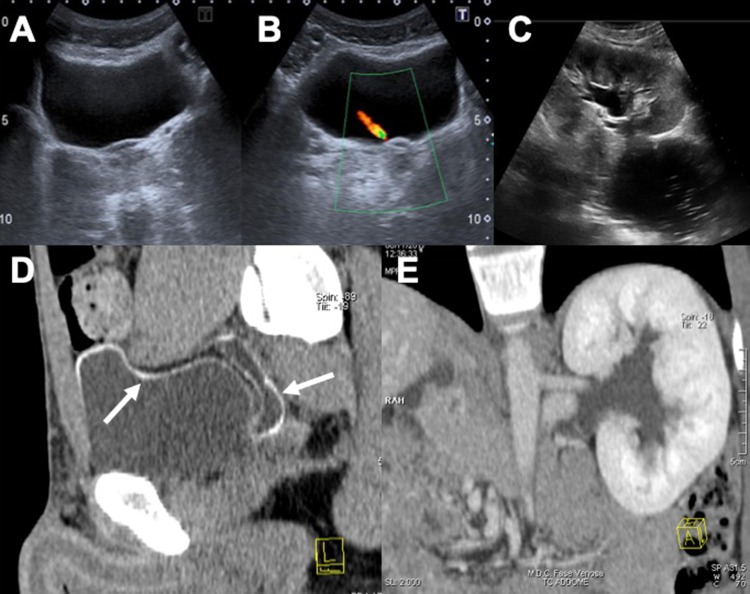
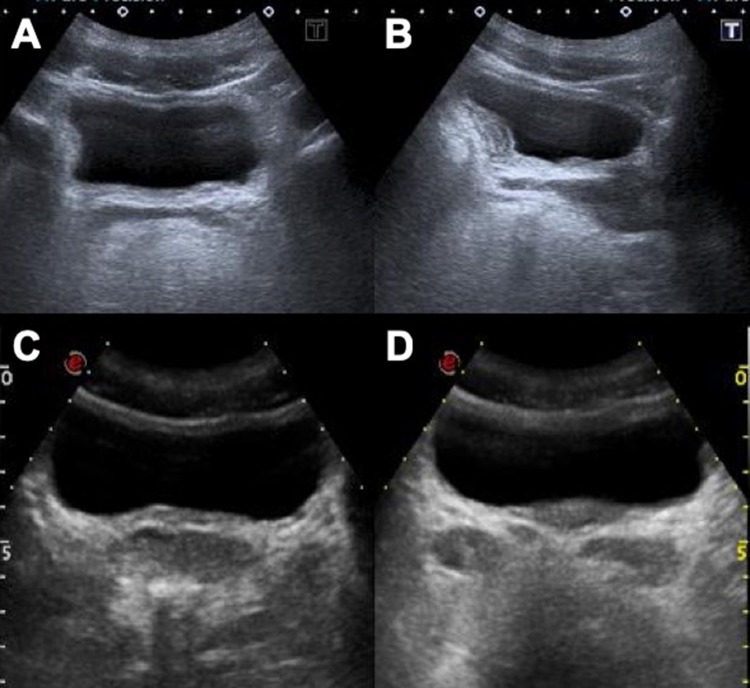
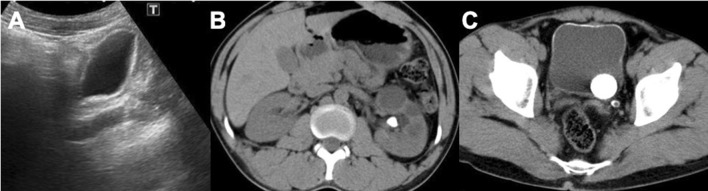
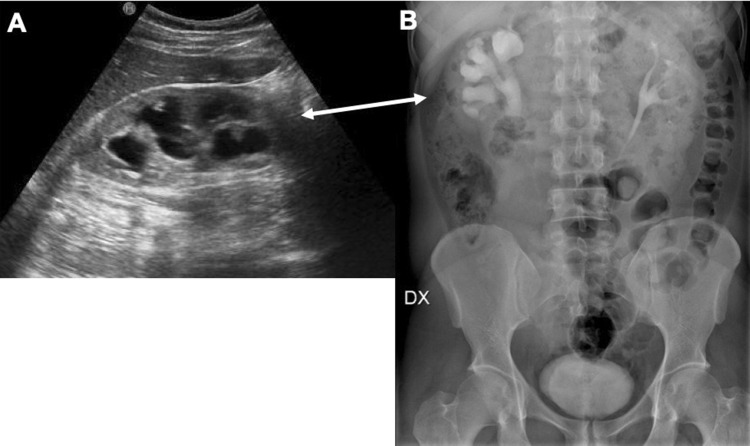
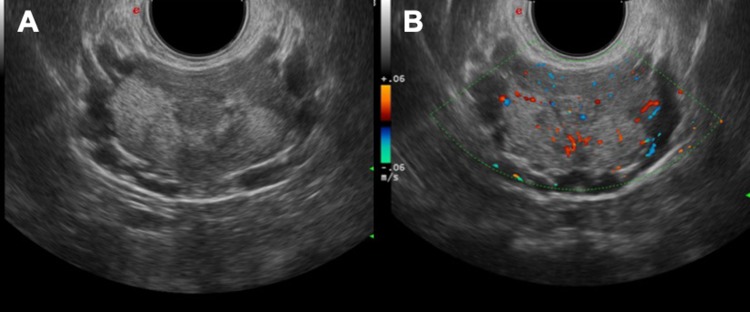
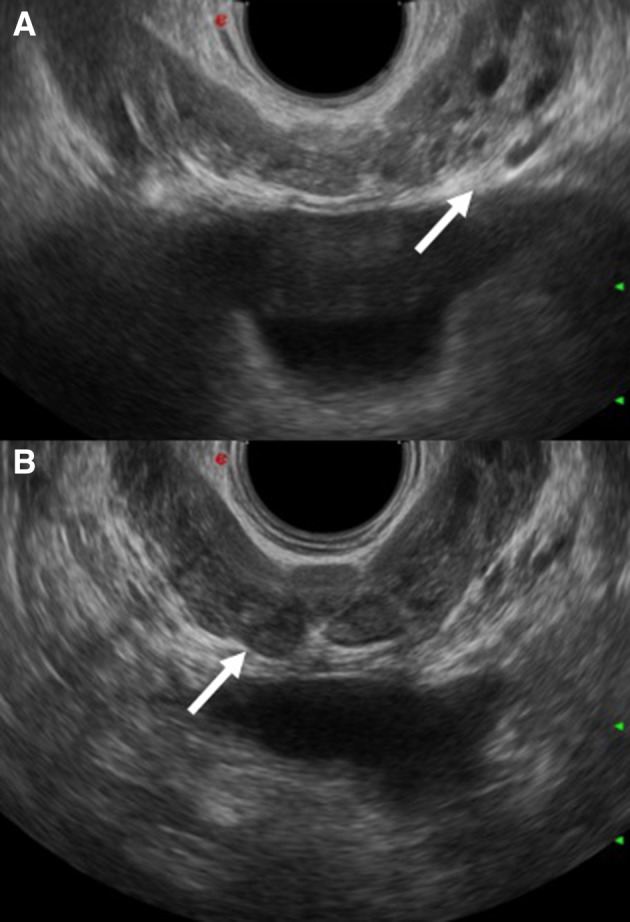
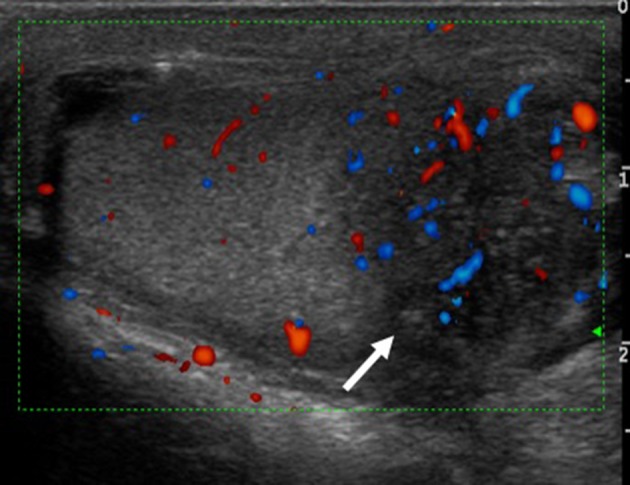
Urogenital schistosomiasis is a parasitic disease caused by S. haematobium which is endemic in tropical and sub-tropical areas but is increasingly diagnosed in temperate non-endemic countries due to migration and international travels. Early identification and treatment of the disease are fundamental to avoid associated severe sequelae such as bladder carcinoma, hydronephrosis leading to kidney failure and reproductive complications. Radiologic imaging, especially through ultrasound examination, has a fundamental role in the assessment of organ damage and follow-up after treatment. Imaging findings of urinary tract schistosomiasis are observed mainly in the ureters and bladder. The kidneys usually appear normal until a late stage of the disease.
Keywords: Bladder; Infection; Kidney; Schistosoma; Ultrasound.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Scarlata F, Giordano S, Romani A, Marasa L, Lipani G, Infurnari L, Titone L. Urinary schistosomiasis: remarks on a case. Infez Med. 2005;13(4):259–264. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
