

Cephalosporin Allergy: Current Understanding and Future Challenges
- PMID: 31495420
- PMCID: PMC6955146
- DOI: 10.1016/j.jaip.2019.06.001
Cephalosporin Allergy: Current Understanding and Future Challenges
Abstract
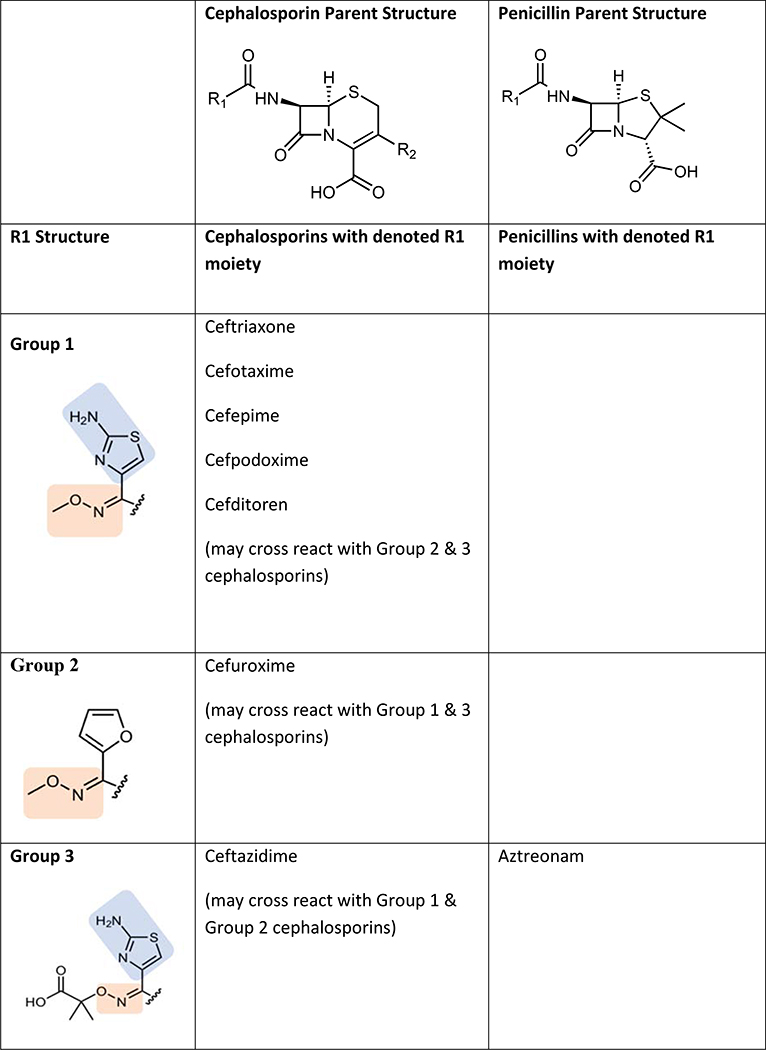
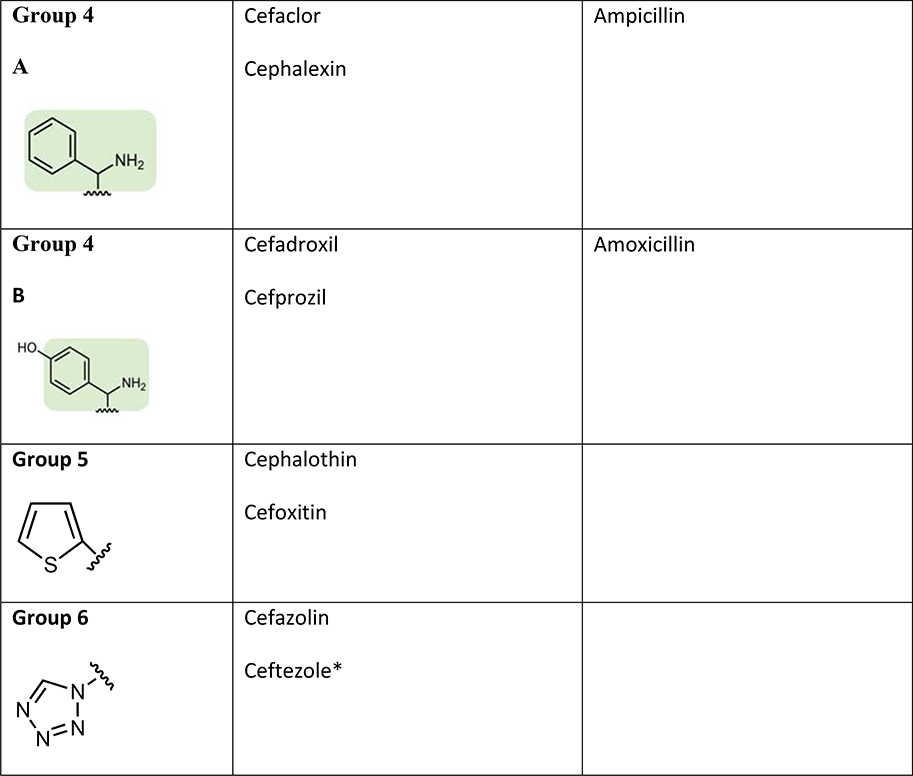
Cephalosporins are commonly used antibiotics both in hospitalized patients and in outpatients. Hypersensitivity reactions to cephalosporins are becoming increasingly common with a wide range of immunopathologic mechanisms. Cephalosporins are one of the leading causes for perioperative anaphylaxis and severe cutaneous adverse reactions. Patients allergic to cephalosporins tend to tolerate cephalosporins with disparate R1 side chains but may react to other beta-lactams with common R1 side chains. Skin testing for cephalosporins has not been well validated but appears to have a good negative predictive value for cephalosporins with disparate R1 side chains. In vitro tests including basophil activation tests have lower sensitivity when compared with skin testing. Rapid drug desensitization procedures are safe and effective and have been used successfully for immediate and some nonimmediate cephalosporin reactions. Many gaps in knowledge still exist regarding cephalosporin hypersensitivity.
Keywords: Allergy; Anaphylaxis; Beta-lactam; Cephalosporin; Cross-reactivity; Penicillin; Skin test.
Copyright © 2019 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Drs. Khan, Banerji, Bernstein, Bilgicer, Castells, Ein, Lang, and Phillips have no relevant conflicts of interest.
Figures
References
-
- Versporten A, Coenen S, Adriaenssens N, Muller A, Minalu G, Faes C, et al. European Surveillance of Antimicrobial Consumption (ESAC): outpatient cephalosporin use in Europe (1997–2009). J Antimicrob Chemother. 2011;66 Suppl 6:vi25–35. - PubMed
-
- Zhou L, Dhopeshwarkar N, Blumenthal KG, Goss F, Topaz M, Slight SP, et al. Drug allergies documented in electronic health records of a large healthcare system. Allergy. 2016;71(9):1305–13. - PubMed
-
- Macy E, Poon KYT. Self-reported antibiotic allergy incidence and prevalence: age and sex effects. Am J Med. 2009;122(8):778 e1–7. - PubMed
-
- Macy E, Contreras R. Adverse reactions associated with oral and parenteral use of cephalosporins: A retrospective population-based analysis. J Allergy Clin Immunol. 2015;135(3):745–52 e5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
