

Systematic review and meta-analysis of esophageal cancer in Africa: Epidemiology, risk factors, management and outcomes
- PMID: 31496629
- PMCID: PMC6710188
- DOI: 10.3748/wjg.v25.i31.4512
Systematic review and meta-analysis of esophageal cancer in Africa: Epidemiology, risk factors, management and outcomes
Abstract
Background: Esophageal cancer (EC) is associated with a poor prognosis, particularly so in Africa where an alarmingly high mortality to incidence ratio prevails for this disease.
Aim: To provide further understanding of EC in the context of the unique cultural and genetic diversity, and socio-economic challenges faced on the African continent.
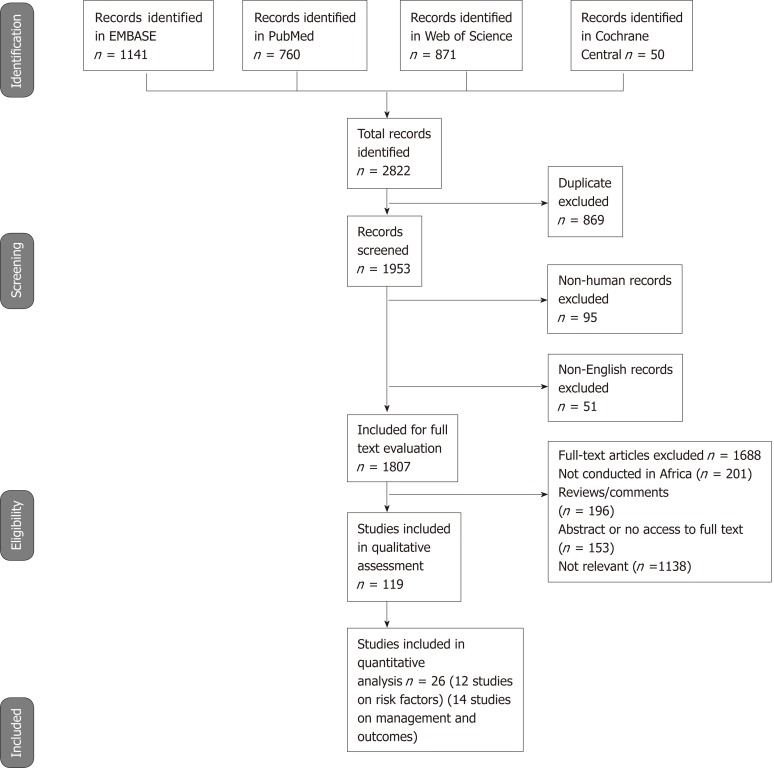
Methods: We performed a systematic review of studies from Africa to obtain data on epidemiology, risk factors, management and outcomes of EC. A non-systematic review was used to obtain incidence data from the International Agency for Research on Cancer, and the Cancer in Sub-Saharan reports. We searched EMBASE, PubMed, Web of Science, and Cochrane Central from inception to March 2019 and reviewed the list of articles retrieved. Random effects meta-analyses were used to assess heterogeneity between studies and to obtain odds ratio (OR) of the associations between EC and risk factors; and incidence rate ratios for EC between sexes with their respective 95% confidence intervals (CI).
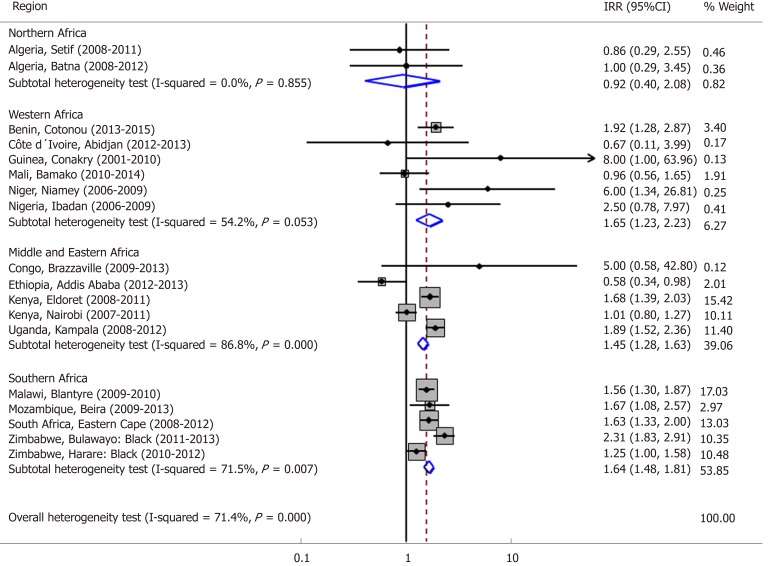
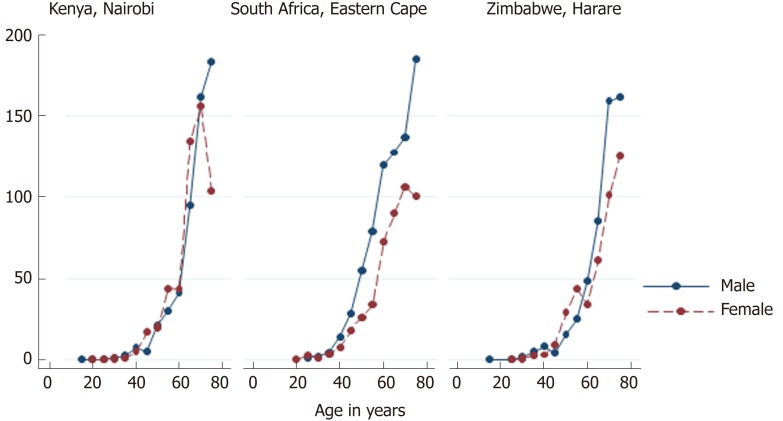
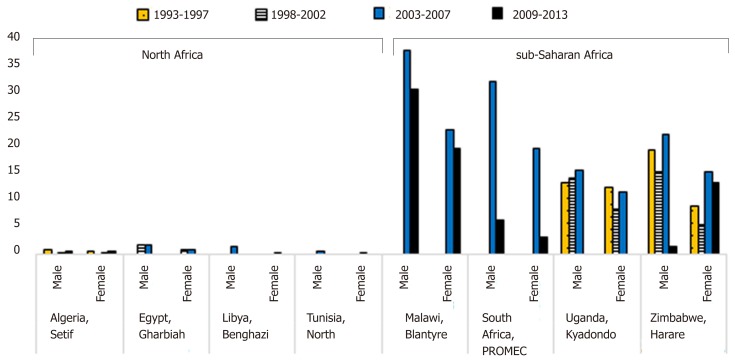
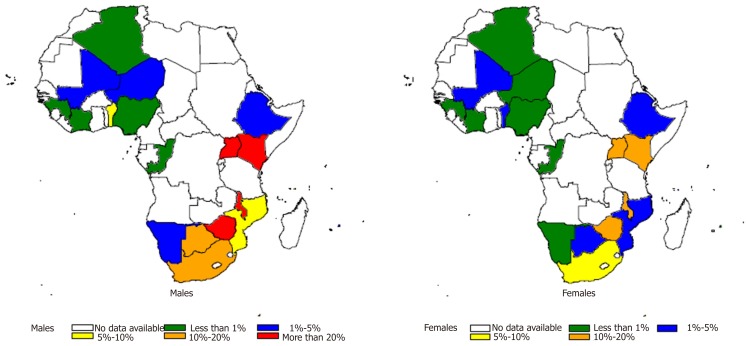
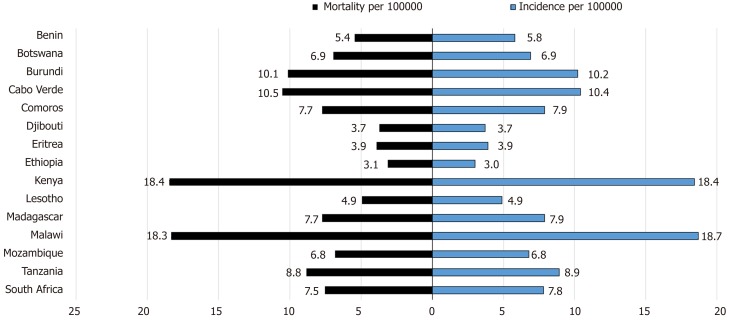
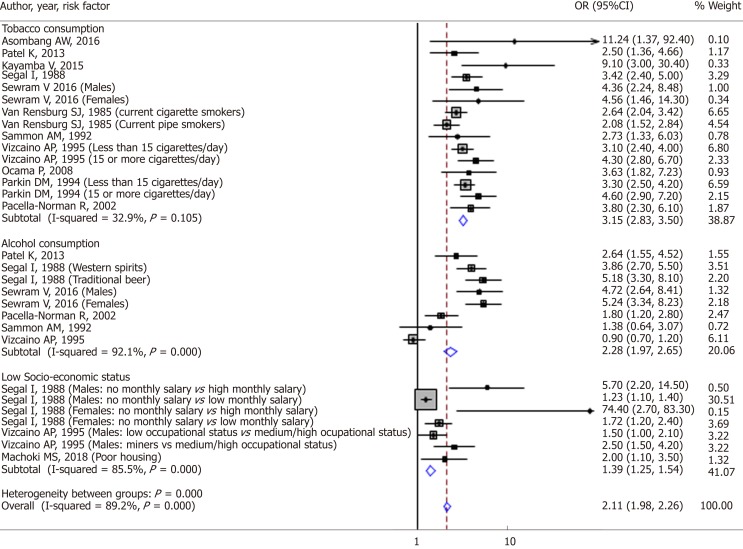
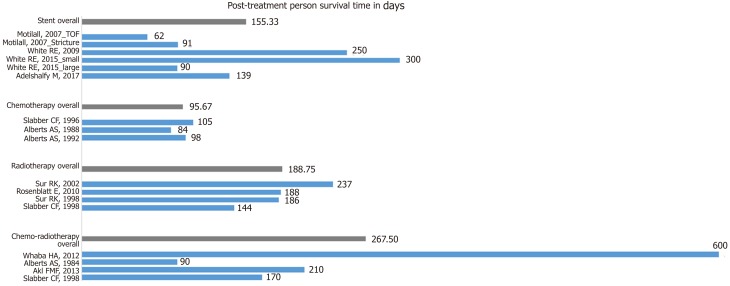
Results: The incidence of EC is higher in males than females, except in North Africa where it is similar for both sexes. The highest age-standardized rate is from Malawi (30.3 and 19.4 cases/year/100000 population for males and females, respectively) followed by Kenya (28.7 cases/year/100000 population for both sexes). The incidence of EC rises sharply after the age of 40 years and reaches a peak at 75 years old. Meta-analysis shows a strong association with tobacco (OR 3.15, 95%CI: 2.83-3.50). There was significant heterogeneity between studies on alcohol consumption (OR 2.28, 95%CI: 1.94-2.65) and on low socioeconomic status (OR 139, 95%CI: 1.25-1.54) as risk factors, but these could also contribute to increasing the incidence of EC. The best treatment outcomes were with esophagectomy with survival rates of 76.6% at 3 years, and chemo-radiotherapy with an overall combined survival time of 267.50 d.
Conclusion: Africa has high incidence and mortality rates of EC, with preventable and non-modifiable risk factors. Men in this setting are at increased risk due to their higher prevalence of tobacco and alcohol consumption. Management requires a multidisciplinary approach, and survival is significantly improved in the setting of esophagectomy and chemoradiation therapy.
Keywords: Cancer in Africa; Esophageal cancer in Africa; Esophageal squamous cell carcinoma; Systematic review.
Conflict of interest statement
Conflict-of-interest statement: All the authors declare that they have no competing interests.
Figures
References
-
- GLOBOCAN 2018: Estimated cancer incidence, mortality and prevalence worldwide in 2018. Available from: http://gco.iarc.fr/today/data/factsheets/cancers/6-Oesophagus-fact-sheet....
-
- Parkin DM. Ferlay J, Hamdi-Cheri M, Sitas F, Thomas JO, Wahunga H, Whelan SL. Cancer in Africa: Epidemiology and Prevention. IARC Scientific Publication, 2003 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
