

Ab interno canaloplasty combined with trabecular bypass stenting in eyes with primary open-angle glaucoma
- PMID: 31496645
- PMCID: PMC6697664
- DOI: 10.2147/OPTH.S215667
Ab interno canaloplasty combined with trabecular bypass stenting in eyes with primary open-angle glaucoma
Abstract
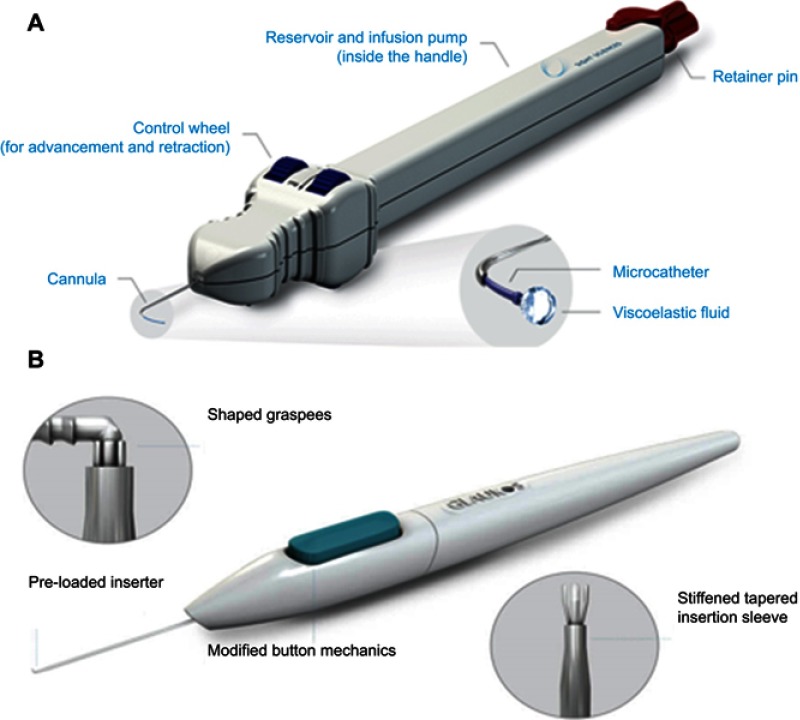
Purpose: Evaluate outcomes of trabecular meshwork (TM) bypass (iStent® GTS100) with cataract extraction (CE) and TM-bypass + ab interno canaloplasty (CP) (VISCO360®) with CE in patients with primary open-angle glaucoma (POAG).
Setting: Private surgical center for a comprehensive ophthalmology practice.
Design: Retrospective analysis of 186 eyes from 130 consecutive patients with 6 months follow-up.
Methods: Eligible eyes had POAG, indicated for CE, and had received CE + TM-bypass or CE + TM-bypass + CP. Exclusions: glaucomas not POAG, SLT within 6 months, or previous ALT. IOP, visual acuity, and medication use assessed at baseline, months 1, 3, and 6. Endpoints were mean reduction in IOP from baseline at 6 months, proportion with IOP reduction at 6 months of ≥20% and IOP <18 mmHg on same or fewer medications, mean medication reduction, and proportion medication independent.
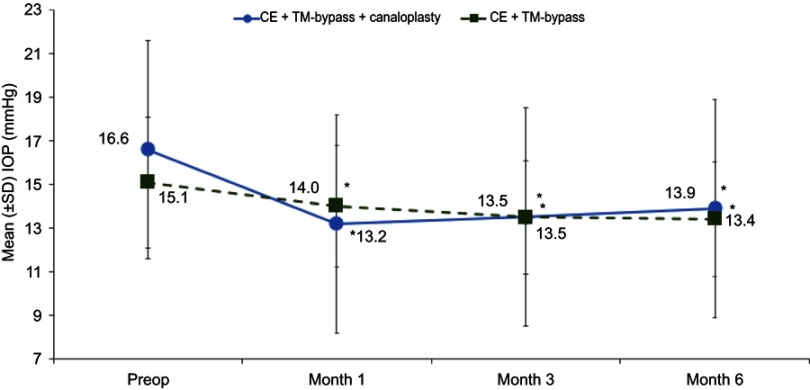
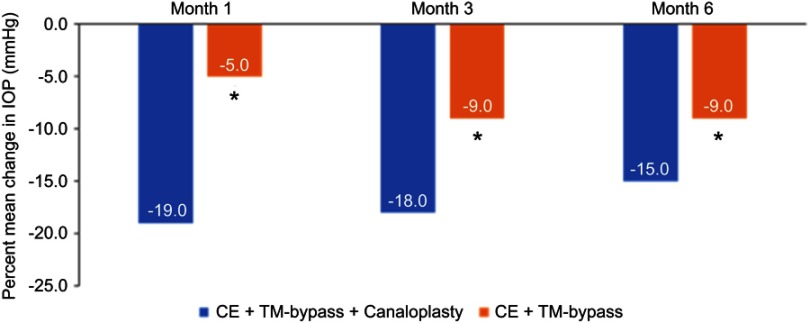
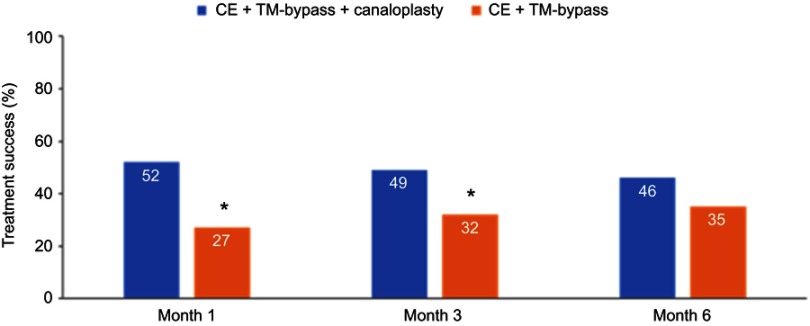
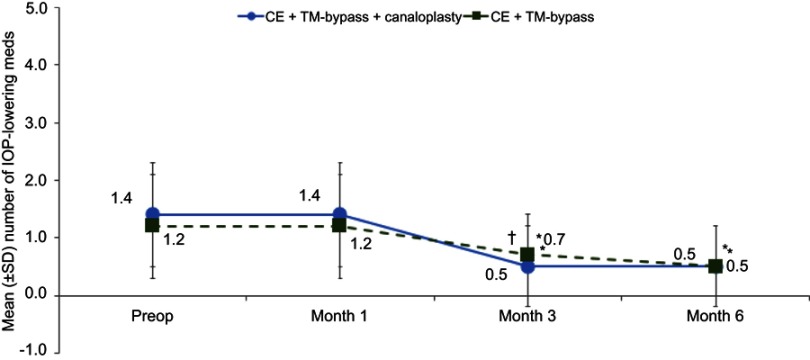
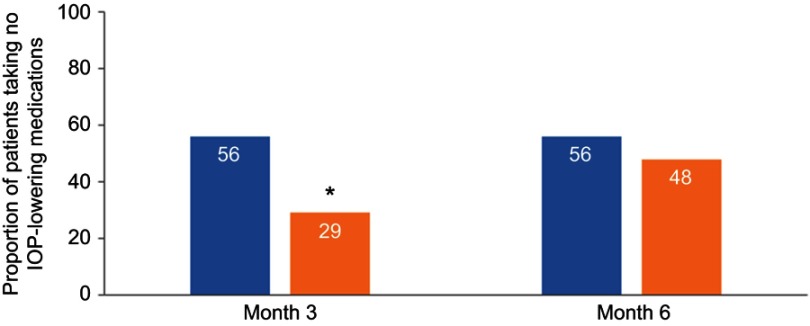
Results: Eighty-six eyes comprised the CE + TM-bypass + CP group; 100 eyes in the CE + TM-bypass group. At 6 months: mean IOP reduction was 2.9±3.6 mmHg for CE + TM-bypass + CP and 1.7±3.1 mmHg for CE + TM-bypass group (P<0.05); the proportion with IOP reduction of ≥20% and an IOP <18 mmHg on the same or fewer medications was 46% for CE + TM-bypass + CP and 35% for CE + TM-bypass; for both CE + TM-bypass + CP and CE + TM-bypass, mean number of medications was decreased (0.9 and 0.7, P<0.0001) with 56% and 48% off all medication. The most common AE were inflammation (6%) for CE + TM-bypass + CP group and VA loss (8%) for CE + TM-bypass.
Conclusion: At six months, a greater proportion of CE + TM-bypass + CP patients achieved IOP reduction of ≥20% and an IOP <18 mmHg on the same or fewer medications than for TM-bypass + CE.
Keywords: 360-degree viscodilation; MIGS; VISCO360®; canaloplasty; glaucoma; viscodilation.
Conflict of interest statement
Mr Marius Heersink reports non-financial support from Sight Sciences, Inc., during the conduct of the study. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
360° ab-interno Schlemm's canal viscodilation in primary open-angle glaucoma.Clin Ophthalmol. 2019 Jul 15;13:1235-1246. doi: 10.2147/OPTH.S203917. eCollection 2019. Clin Ophthalmol. 2019. PMID: 31409962 Free PMC article.
-
Circumferential Viscodilation Ab Interno Combined with Phacoemulsification for Treatment of Open-Angle Glaucoma: 12-Month Outcomes.Clin Ophthalmol. 2020 May 20;14:1357-1364. doi: 10.2147/OPTH.S252965. eCollection 2020. Clin Ophthalmol. 2020. PMID: 32546943 Free PMC article.
-
Clinical Results of Ab Interno Canaloplasty in Patients with Open-Angle Glaucoma.Clin Ophthalmol. 2020 Oct 29;14:3641-3650. doi: 10.2147/OPTH.S275087. eCollection 2020. Clin Ophthalmol. 2020. PMID: 33154624 Free PMC article.
-
Ab interno trabecular bypass surgery with Trabectome for open-angle glaucoma.Cochrane Database Syst Rev. 2021 Feb 4;2(2):CD011693. doi: 10.1002/14651858.CD011693.pub3. Cochrane Database Syst Rev. 2021. PMID: 33580495 Free PMC article.
-
Ab interno trabecular bypass surgery with iStent for open-angle glaucoma.Cochrane Database Syst Rev. 2019 Mar 28;3(3):CD012743. doi: 10.1002/14651858.CD012743.pub2. Cochrane Database Syst Rev. 2019. PMID: 30919929 Free PMC article.
Cited by
-
Efficacy and Safety of Cataract Surgery Combined with Ab Interno Canaloplasty and Micro-Trabecular Bypass Stent Surgery in Open-Angle Glaucoma.Clin Ophthalmol. 2025 Feb 11;19:469-481. doi: 10.2147/OPTH.S504247. eCollection 2025. Clin Ophthalmol. 2025. PMID: 39959880 Free PMC article.
-
Visual Function After Schlemm's Canal-Based MIGS.J Clin Med. 2025 Apr 7;14(7):2531. doi: 10.3390/jcm14072531. J Clin Med. 2025. PMID: 40217980 Free PMC article. Review.
-
Meta-Analysis of MINIject vs. Two iStents as Standalone Treatment for Glaucoma with 24 Months of Follow-Up.J Clin Med. 2024 Dec 17;13(24):7703. doi: 10.3390/jcm13247703. J Clin Med. 2024. PMID: 39768626 Free PMC article. Review.
-
Comparative Effectiveness and Safety of Two Different Trabecular MIGS Devices With and Without Ab Interno Canaloplasty in Patients with Primary Open-Angle Glaucoma.Ophthalmol Ther. 2023 Dec;12(6):3307-3322. doi: 10.1007/s40123-023-00819-5. Epub 2023 Oct 6. Ophthalmol Ther. 2023. PMID: 37801274 Free PMC article.
-
Minimally Invasive Glaucoma Surgery: Safety of Individual Devices.J Clin Med. 2022 Nov 18;11(22):6833. doi: 10.3390/jcm11226833. J Clin Med. 2022. PMID: 36431310 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
