

Augmented renal clearance is associated with inadequate antibiotic pharmacokinetic/pharmacodynamic target in Asian ICU population: a prospective observational study
- PMID: 31496765
- PMCID: PMC6701640
- DOI: 10.2147/IDR.S213183
Augmented renal clearance is associated with inadequate antibiotic pharmacokinetic/pharmacodynamic target in Asian ICU population: a prospective observational study
Abstract
Background: Augmented renal clearance (ARC) is common in critically ill patients and could result in subtherapeutic antibiotic concentration. However, data in the Asian population are still lacking. The aim of this study was to explore the incidence and risk factors of ARC and its effect on β-lactam pharmacokinetics/pharmacodynamics (PK/PD) in Asian populations admitted to a medical ICU. In addition, we evaluated the appropriateness of using three estimated glomerular filtration (eGFR) formulas [Cockcroft-Gault (CG), Modification of Diet in Renal Disease (MDRD), and the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI)] as screening tools.
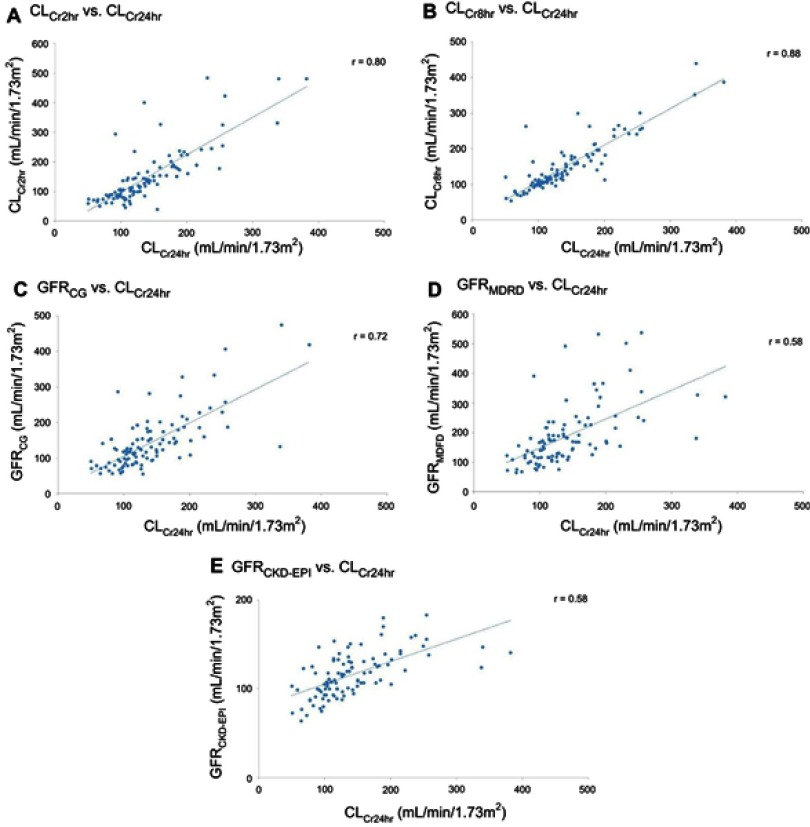
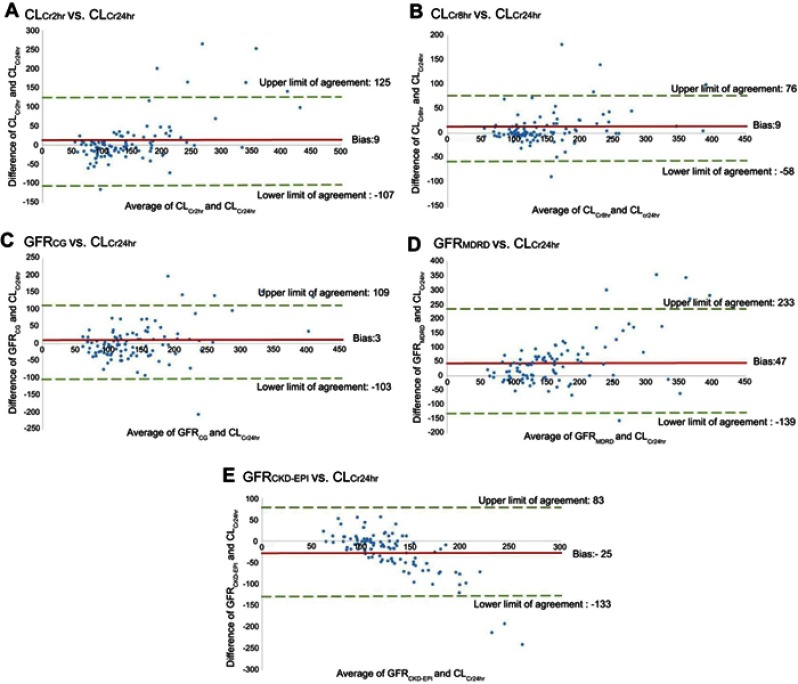
Methods: We measured 2-, 8-, and 24-hr creatinine clearance (CLCr) and calculated eGFR by using three formulas for each. ARC was defined as CLCr24hr >130 mL/min/1.73 m2. Concentrations at the mid-dosing interval and prior to the next dose were collected if patients received the β-lactam antibiotic of piperacillin/tazobactam, cefepime, and meropenem, to determine the PK/PD index of fT > MIC. Multiple logistic regression analysis was conducted to identify the risk factors for ARC. Pearson correlation coefficient and the Bland and Altman method were applied to assess the accuracy of CLCr2hr, CLCr8hr, and eGFR for predicting ARC.
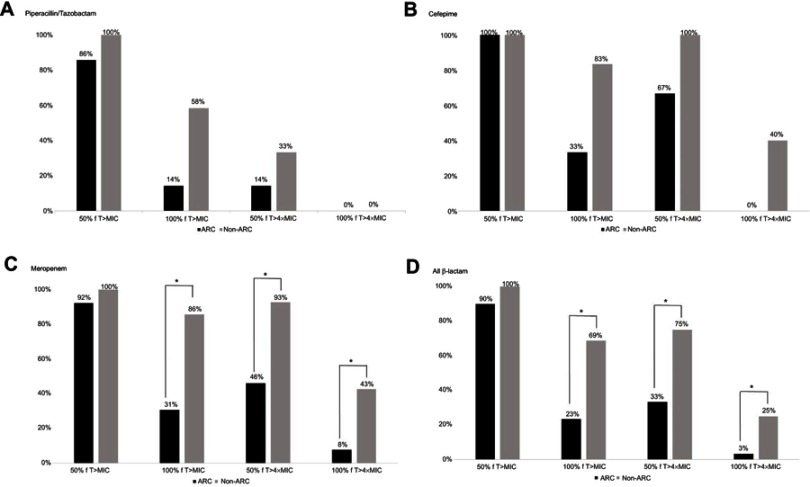
Results: Of 100 patients, 46 (46%) manifested ARC. Younger age (<50 years) and lower Sequential Organ Failure Assessment score increased the likelihood of ARC. ARC resulted in a low chance of achieving 50% fT >4MIC (33% vs 75%, p<0.01), 100% fT > MIC (23% vs 69%, p<0.01), and 100% fT >4MIC (3% vs 25%, p<0.02). CLCr8hr wielded the best correlation and agreement with CLCr24hr. eGFRCG was the most appropriate screening tool, and the optimal cutoff value for detecting ARC was 130.5 mL/min/1.73 m2.
Conclusion: ARC is associated with inadequate β-lactam PK/PD target in Asian ICU.
Keywords: augmented renal clearance (ARC); critical care; glomerular filtration rate; pharmacokinetic/pharmacokinetics; β-lactam antibiotic.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
-
- Carrie C, Petit L, d’Houdain N, et al. Association between augmented renal clearance, antibiotic exposure and clinical outcome in critically ill septic patients receiving high doses of beta-lactams administered by continuous infusion: a prospective observational study. Int J Antimicrob Agents. 2018;51(3):443–449. doi: 10.1016/j.ijantimicag.2017.11.013 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
