

Sleep disturbances in patients with amyotrophic lateral sclerosis: current perspectives
- PMID: 31496852
- PMCID: PMC6701267
- DOI: 10.2147/NSS.S183504
Sleep disturbances in patients with amyotrophic lateral sclerosis: current perspectives
Abstract
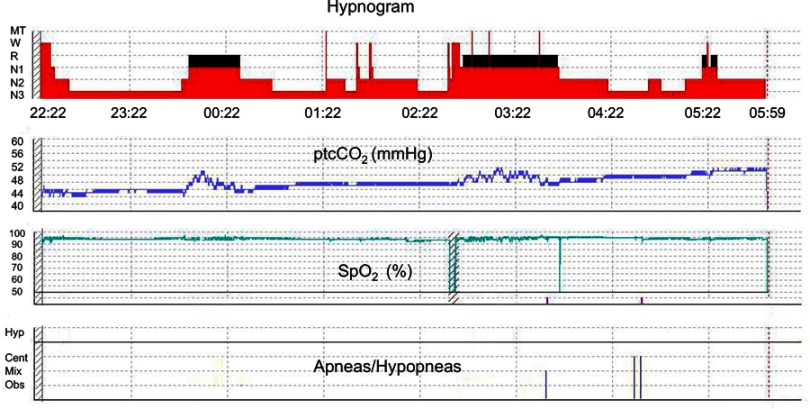
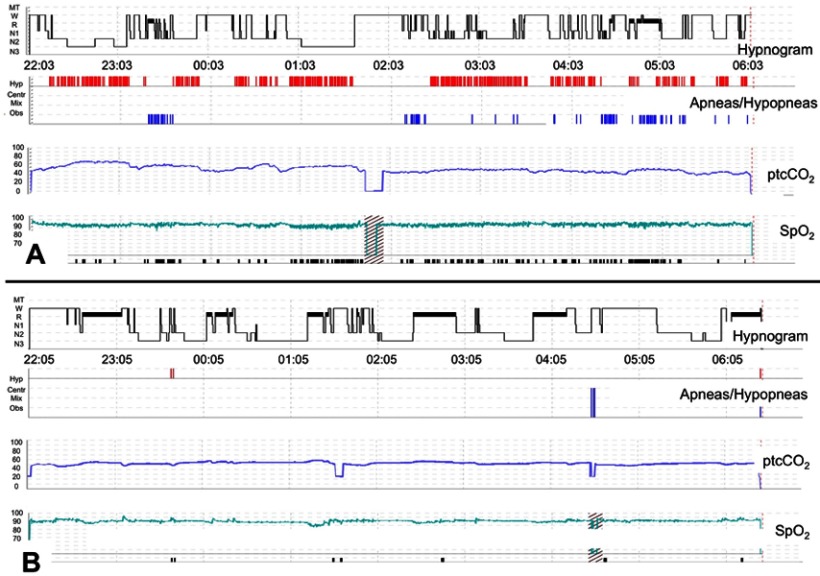
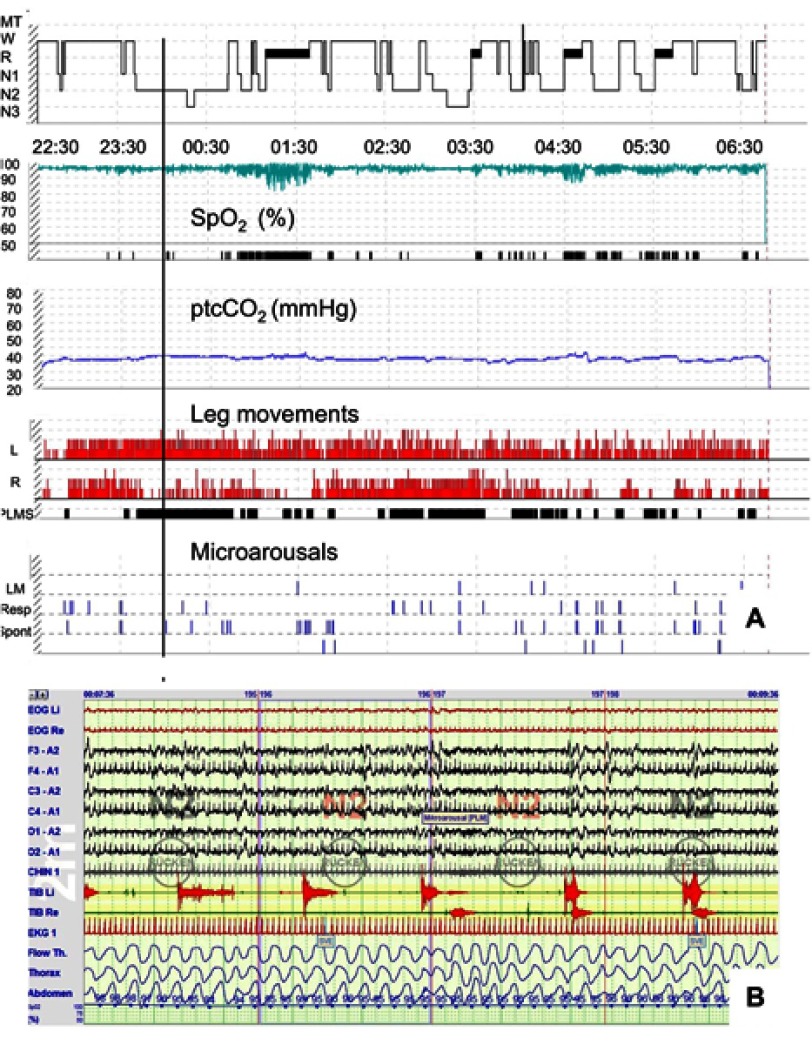
Amyotrophic lateral sclerosis (ALS) is a progressive motor neuron disease inevitably leading to generalized muscle weakness and premature death. Sleep disturbances are extremely common in patients with ALS and substantially add to the burden of disease for both patients and caregivers. Disruption of sleep can be caused by physical symptoms, such as muscle cramps, pain, reduced mobility, spasticity, mucus retention, and restless legs syndrome. In addition, depression and anxiety may lead to significant insomnia. In a small subset of patients, rapid eye movement (REM) sleep behavioral disorder may be present, reflecting neurodegeneration of central nervous system pathways which are involved in REM sleep regulation. With regard to overall prognosis, sleep-disordered breathing (SDB) and nocturnal hypoventilation (NH) are of utmost importance, particularly because NH precedes respiratory failure. Timely mechanical ventilation is one of the most significant therapeutic measures to prolong life span in ALS, and transcutaneous capnometry is superior to pulse oxymetry to detect NH early. In addition, it has been shown that in patients on home ventilatory support, survival time depends on whether normocapnia, normoxia, and elimination of apneic events during sleep can be reliably achieved. Several studies have investigated sleep patterns and clinical determinants of sleep disruption in ALS, but exact prevalence numbers are unknown. Thus, constant awareness for sleep-related symptoms is appropriate. Since no curative treatment can be offered to affected patients, sleep complaints should be thoroughly investigated in order to identify any treatable etiology and improve or stabilize quality of life as much as possible. The use of hypnotics should be confined to palliation during the terminal phase and refractory insomnia in earlier stages of the disease, taking into account that most compounds potentially aggravate SDB.
Keywords: amyotrophic lateral sclerosis; health-related quality of life; non-invasive ventilation; sleep disorders; sleep-disordered breathing.
Conflict of interest statement
Dr Matthias Boentert reports grants from Sanofi-Genzyme GmbH and Loewenstein Medical GmbH, outside the submitted work, and no other conflicts of interest in this work.
Figures
References
-
- Mizutani T, Aki M, Shiozawa R, et al. Development of ophthalmoplegia in amyotrophic lateral sclerosis during long-term use of respirators. J Neurol Sci. 1990;99(2–3):311–319. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
