

Evaluation of Neutrophil-lymphocyte and Platelet-lymphocyte Ratios as Predictors of 30-day Mortality in Patients Hospitalized for an Episode of Acute Decompensated Heart Failure
- PMID: 31496909
- PMCID: PMC6708303
- DOI: 10.2478/jomb-2018-0044
Evaluation of Neutrophil-lymphocyte and Platelet-lymphocyte Ratios as Predictors of 30-day Mortality in Patients Hospitalized for an Episode of Acute Decompensated Heart Failure
Abstract
Background: To investigate the association between both neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) and 30-day mortality in patients hospitalized for an episode of acute decompensated heart failure (ADHF).
Methods: 439 patients admitted to emergency department (ED) for an episode of ADHF. Clinical history, demographic, clinical and laboratory data recorded at ED admission and then correlated with 30-day mortality.
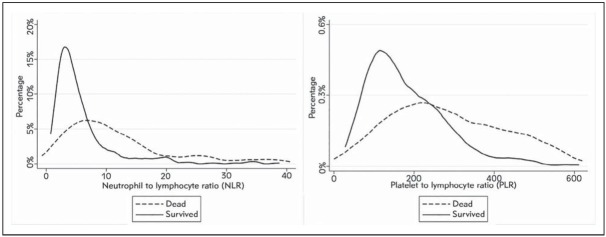
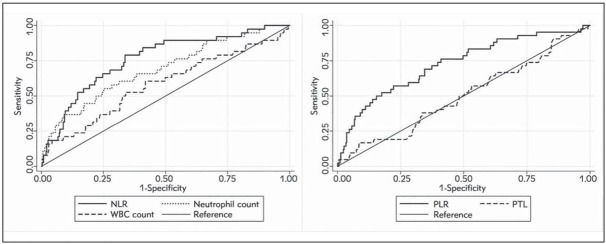
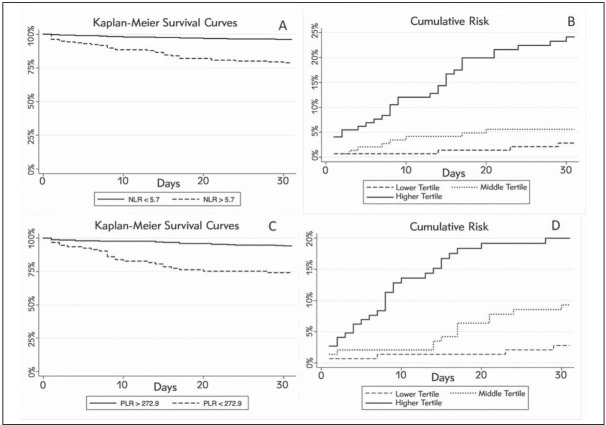
Results: 45/439 (10.3%) patients died within 30 days from ED admission. The median values of NLR (4.1 vs 11.7) and PLR (159.1 vs 285.9) were significantly lower in survivors than in patients who died. The area under the ROC curve of NLR was significantly higher than that of the neutrophil count (0.76 vs 0.59; p<0.001), whilst the AUC of PLR was significantly better than that of the platelet count (0.71 vs 0.51; p<0.001). In univariate analysis, both NLR and PLR were significantly associated with 30-day. In the fully-adjusted multivariate model, NLR (odds ratio, 3.63) and PLR (odds ratio, 3.22) remained independently associated with 30-day mortality after ED admission.
Conclusions: Routine assessment of NLR and PLR at ED admission may be a valuable aid to complement other conventional measures for assessing the medium-short risk of ADHF patients.
Uvod: Svrha rada je bila da se ispitaju odnosi povezanosti između neutrofila prema limfocitima (NLR) i trombocita prema limfocitima (PLR) i 30-dnevna smrtnost kod pacijenata koji su hospitalizovani zbog akutnog dekompenzovanog srčanog oštećenja (ADHF).
Metode: U odeljenje hitne medicine (ED) primljeno je 439 pacijenata sa ADHF. Istorija bolesti, demografski i laboratorijski podaci su praćeni prilikom prijema u ED i upoređivani su sa 30-dnevnom smrtnošću.
Rezultati: U toku 30 dana od prijema u ED umrlo je 45/439 (10,33%) pacijenata. Srednje vrednosti NLR (4,11 vs, 11,7) i PLR (159,1 vs 285,9) bile su značajno niže kod preživelih u odnosu na preminule pacijente. Površina ispod ROC krive u NLR bila je značajno viša nego kod iste u broju neutrofila (0,76 vs 0,59; p < 0,001), dok je AUC u slučaju PLR bio značajno bolji nego u odnosu na broj trombocita (0,71 vs 0,51; p < 0,001). Univarijantne analize u slučaju oba NLR iPLR bile su značajno povezane za 30-danom. U potpuno podešenom multivarijantnom modelu, NLR (Odds odnos, 2,63) i PLR (Odds odnos, 3,22) bili su nezavisno povezani sa 30-dnevnom smrtnošću posle prijema u ED.
Zaključak: Rutinsko praćenje NLR i PLR pri ED prijemu može da bude veoma značajna pomoć uz druga konvencionalna merenja i praćenja radi umanjenja rizika kod ADHF pacijenata.
Keywords: acute heart failure; lymphocytes; monocytes; mortality; platelets.
Conflict of interest statement
Conflict of interest Conflict of interest statement: The authors stated that they have no conflicts of interest regarding the publication of this article.
Figures
References
-
- Sperry BW, Ruiz G, Najjar SS. Hospital readmission in heart failure, a novel analysis of a longstanding problem. Heart Fail Rev. 2015;20:251–8. - PubMed
-
- Rørth R, Fosbøl EL, Mogensen UM. Employment status at time of first hospitalization for heart failure is associated with a higher risk of death and rehospitalization for heart failure. Eur J Heart Fail. 2018;20(2):240–47. - PubMed
-
- Briasoulis A, Androulakis E, Christophides T. The role of inflammation and cell death in the pathogenesis, progression and treatment of heart failure. Heart Fail Rev. 2016;2:169–76. - PubMed
LinkOut - more resources
Full Text Sources