

Melanoacanthoma Masquerading as Melanoma: Case Reports and Literature Review
- PMID: 31497429
- PMCID: PMC6707823
- DOI: 10.7759/cureus.4998
Melanoacanthoma Masquerading as Melanoma: Case Reports and Literature Review
Abstract
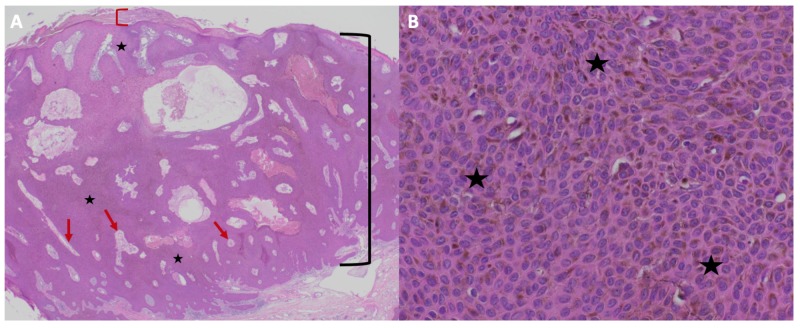
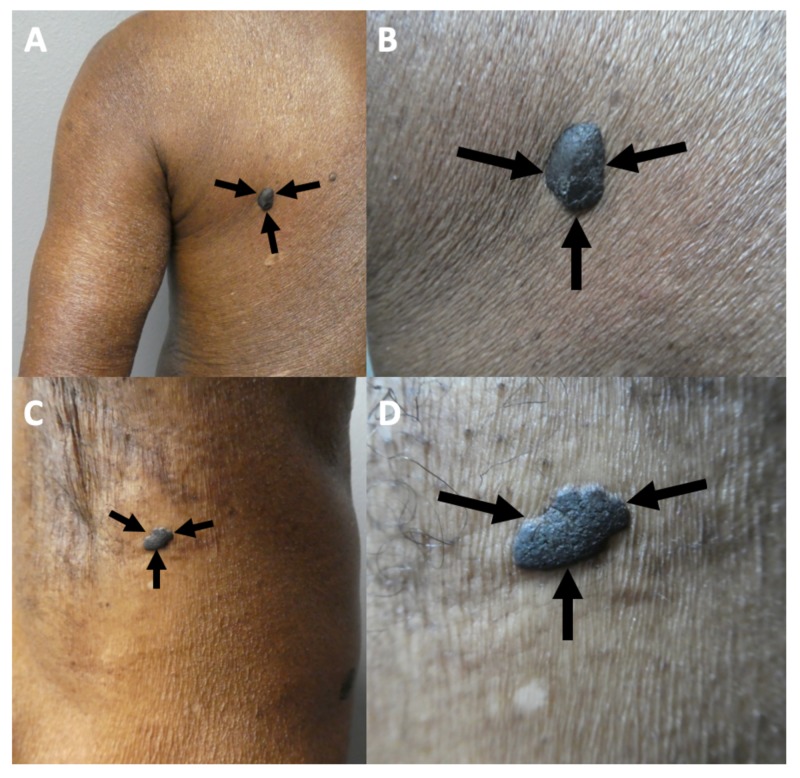
Melanoacanthoma is a benign epithelial tumor composed of melanocytes and keratinocytes that can morphologically mimic malignant neoplasms. Two patients with melanoacanthoma that clinically masqueraded as melanoma are described: a 65-year-old African-American woman with a pigmented nodule on the right preauricular area and an 85-year-old Haitian-Creole man with a large exophytic nodule on his left lower abdomen. Melanoma was clinically suspected in both patients. Biopsies were performed, which established the diagnosis of melanoacanthoma. Complete removal of a melanoacanthoma should be considered since partial excision may result in recurrence.
Keywords: malignant; melanoacanthoma; melanoma; pigmented melanocyte.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
-
- Clinical and dermoscopic features of cutaneous melanoacanthoma. Chung E, Marghoob A, Carrera C, et al. JAMA Dermatol. 2015;151:1129–1130. - PubMed
-
- Benign mixed tumors of melanocytes and malpighian cells. Mishima Y, Pinkus H. AMA Arch Dermatol. 1960;81:539–550. - PubMed
-
- Melanoacanthoma: ultrastructural and immunological studies. Schlappner OL, Rowden G, Philips TM, Rahim Z. J Cutan Pathol. 1978;5:127–141. - PubMed
Publication types
LinkOut - more resources
Full Text Sources