

Evaluation of crystal violet decolorization assay and resazurin microplate assay for antimycobacterial screening
- PMID: 31497667
- PMCID: PMC6722264
- DOI: 10.1016/j.heliyon.2019.e02263
Evaluation of crystal violet decolorization assay and resazurin microplate assay for antimycobacterial screening
Abstract
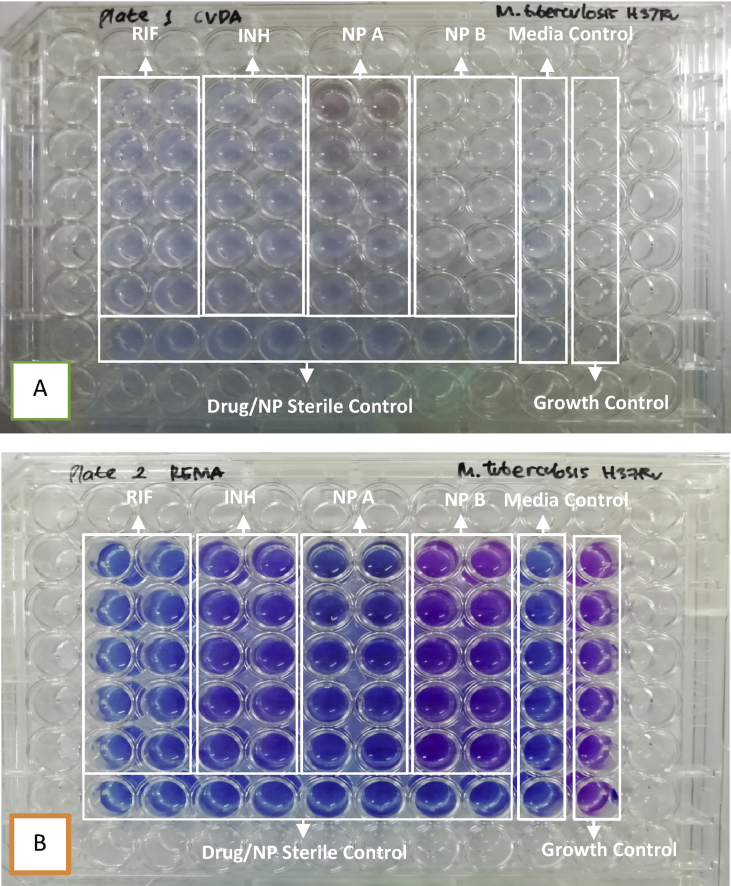
The main obstacle in antimycobacterial discovery is the extremely slow growth rates of pathogenic mycobacteria that lead to the long incubation times needed in antimycobacterial screening. Some in vitro testings has been developed and are currently available for antimycobacterial screening. The aim of the study was to compare Resazurin Microplate Assay (REMA) and Crystal Violet Decolorization Assay (CVDA) for testing mycobacteria susceptibility to isoniazid and rifampicin as well as for antimycobacterial screening of natural products (NP). Mycobacterium tuberculosis strain H37Rv and Mycobacterium smegmatis strain mc2 155 were used as tested mycobacteria. Serial two-fold dilutions from 0.0625 to 1.0 μg/mL for the isoniazid and rifampicin and from 6.25 to 100.0 μg/mL for the NP A and B were prepared. Tested mycobacteria were then incubated with tested drugs or NPs in each growth medium at 37 °C for 7 days for M. tuberculosis and 3 days for M. smegmatis. MIC values against M. tuberculosis were interpreted 24-48 h after adding resazurin or at least 72 h after adding crystal violet, whereas MIC values against M. smegmatis were interpreted 1 h after adding resazurin or 24 h after adding crystal violet. The MIC values against M. tuberculosis interpreted by REMA were 0.0625, 0.0625, 6.25, and >100 μg/mL for rifampicin, isoniazid, NP A, and NP B, respectively, and those interpreted by CVDA were 0.0625, 0.0625, 6.25, and >100 μg/mL for rifampicin, isoniazid, NP A, and NP B, respectively. Moreover, the MIC values against M. smegmatis interpreted by REMA were 0.0625, >1, 6.25, and 100 μg/mL for rifampicin, isoniazid, NP A, and NP B, respectively, and those interpreted by CVDA were 0.125, >1, 6.25, and >100 μg/mL for rifampicin, isoniazid, NP A, NP B respectively. In conclusion, REMA is faster and easier than CVDA to interpret MIC values, however CVDA produces higher MIC values than REMA for rifampicin and NP B in M. smegmatis susceptibility testing. Therefore, REMA and CVDA can be used for antimycobacterial screening.
Keywords: Antimicrobial susceptibility testing; Crystal violet decolorization assay; Mycobacterium; Natural product screening; Resazurin microplate assay.
Figures

References
-
- Affolabi D., Sanoussi N.D., Odoun M., Martin A., Koukpemedji L., Palomino J.C., Kestens L., Anagonou S., Portaels F. Rapid low-cost identification of Mycobacterium tuberculosis complex using p-nitro-benzoic acid (PNB) as inhibitor and the resazurin microplate assay (REMA): a preliminary study. Afr. J. Microbiol. Res. 2013;7(24):3135–3138.
-
- Altaf M., Miller C.H., Bellows D.S., O'Toole R. Evaluation of the Mycobacterium smegmatis and BCG models for the discovery of Mycobacterium tuberculosis inhibitors. Tuberculosis. 2010;90(6):333–337. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
