

Serum lipoprotein(a) and risk of hemorrhagic stroke among incident peritoneal dialysis patients: a large study from a single center in China
- PMID: 31498021
- PMCID: PMC6746282
- DOI: 10.1080/0886022X.2019.1659151
Serum lipoprotein(a) and risk of hemorrhagic stroke among incident peritoneal dialysis patients: a large study from a single center in China
Abstract
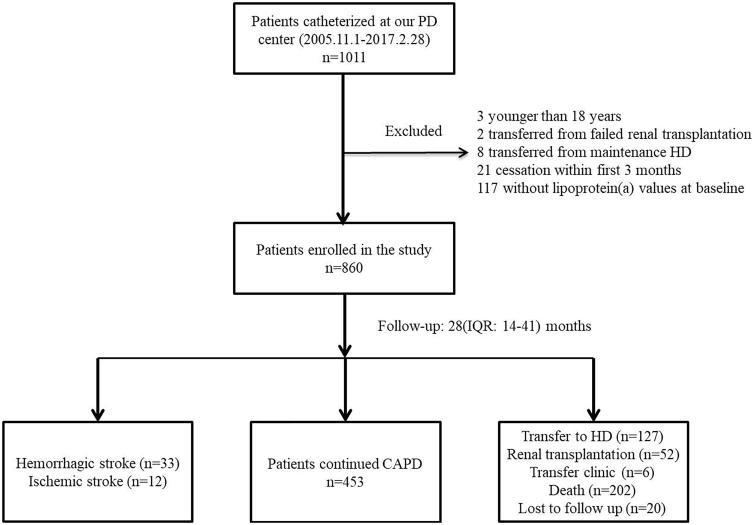
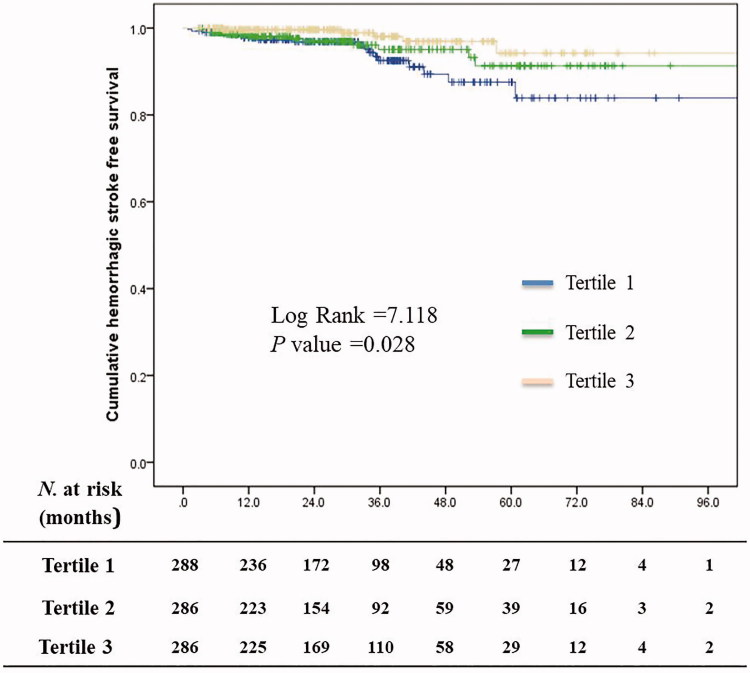
Background: This retrospective study investigated whether baseline serum lipoprotein(a) (Lp(a)) may predict subsequent stroke in patients under chronic peritoneal dialysis (PD). Methods: Eight hundred and sixty incident PD patients, treated from 1 November 2005 to 28 February 2017, were enrolled, and followed until discontinuation of PD, death, or 31 May 2017. Hemorrhagic or ischemic stroke was the primary outcome. The population was stratified by baseline serum Lp(a) tertile. The risk of each stroke subtype was analyzed using the Cox proportional hazard models. Adjustments were made for: age; gender; history of stroke and hypertension; systolic blood pressure; lipid-lowering, antiplatelet and antihypertensive medications; laboratory profiles including hemoglobin, serum albumin, calcium, triglyceride, total and low-density lipoprotein cholesterol; and apolipoprotein A1. Results: Among the 860 participants, 19.3% and 4.1% had diabetes mellitus and a history of stroke, respectively. The median baseline serum Lp(a) was 328 (172-585) mg/L. After 28 (14-41) months of follow-up, 33 (3.84%) and 12 (1.40%) patients developed hemorrhagic and ischemic stroke, respectively. Participants in the highest Lp(a) tertile had a significantly lower risk of hemorrhagic stroke compared with those in the lowest tertile (hazard ratio (HR) 0.3, 95% confidence interval (CI) 0.1-0.86; p = .026); the rates of ischemic stroke were comparable among the tertiles. Each 10 mg/L rise in serum Lp(a) was associated with a 2% (95% CI 0.96-1; p = .033) lower risk of hemorrhagic stroke. Conclusions: Among patients with incident PD, a higher serum Lp(a) level may predict a lower risk of hemorrhagic stroke.
Keywords: End-stage renal disease; hemorrhagic stroke; lipoprotein(a); peritoneal dialysis; stroke.
Figures
Similar articles
-
Serum lipoprotein(a) and risk of mortality in patients on peritoneal dialysis.J Clin Lipidol. 2020 Mar-Apr;14(2):252-259. doi: 10.1016/j.jacl.2020.01.008. Epub 2020 Jan 25. J Clin Lipidol. 2020. PMID: 32081604
-
Prevalence and Impact on Stroke in Patients Receiving Maintenance Hemodialysis versus Peritoneal Dialysis: A Prospective Observational Study.PLoS One. 2015 Oct 20;10(10):e0140887. doi: 10.1371/journal.pone.0140887. eCollection 2015. PLoS One. 2015. PMID: 26485155 Free PMC article.
-
Risk of stroke in long-term dialysis patients compared with the general population.Am J Kidney Dis. 2014 Apr;63(4):604-11. doi: 10.1053/j.ajkd.2013.10.013. Epub 2013 Nov 26. Am J Kidney Dis. 2014. PMID: 24290244
-
Comparison of risk of stroke in patients treated with peritoneal dialysis and hemodialysis: a systematic review and meta-analysis.Ren Fail. 2019 Nov;41(1):650-656. doi: 10.1080/0886022X.2019.1632210. Ren Fail. 2019. PMID: 31296101 Free PMC article.
-
Lipoprotein (a) level as a risk factor for stroke and its subtype: A systematic review and meta-analysis.Sci Rep. 2021 Aug 2;11(1):15660. doi: 10.1038/s41598-021-95141-0. Sci Rep. 2021. PMID: 34341405 Free PMC article.
Cited by
-
Association between lipoprotein (a) and risk of atherosclerotic cardiovascular disease events among maintenance hemodialysis patients in Beijing, China: a single-center, retrospective study.BMC Nephrol. 2024 Aug 1;25(1):250. doi: 10.1186/s12882-024-03690-z. BMC Nephrol. 2024. PMID: 39090533 Free PMC article.
-
Current Trends Featuring the Bridge Between Stroke and End-Stage Renal Disease: A Review.Cureus. 2020 Jul 30;12(7):e9484. doi: 10.7759/cureus.9484. Cureus. 2020. PMID: 32874811 Free PMC article. Review.
-
Risk factors for intracerebral hemorrhage in patients undergoing maintenance hemodialysis.Front Neurol. 2023 Mar 22;14:1111865. doi: 10.3389/fneur.2023.1111865. eCollection 2023. Front Neurol. 2023. PMID: 37034079 Free PMC article.
-
Inverse Association of Lipoprotein(a) on Long-Term Bleeding Risk in Patients with Coronary Heart Disease: Insight from a Multicenter Cohort in Asia.Thromb Haemost. 2024 Jul;124(7):684-694. doi: 10.1055/s-0043-1771188. Epub 2023 Jul 24. Thromb Haemost. 2024. PMID: 37487540 Free PMC article.
References
-
- Ishikawa S, Kotani K, Kario K, et al. . Inverse association between serum lipoprotein(a) and cerebral hemorrhage in the Japanese population. Thromb Res. 2013;131:e54–e58. - PubMed
-
- Kim H, Kim KH, Ahn SV, et al. . Risk of major cardiovascular events among incident dialysis patients: a Korean national population-based study. Int J Cardiol. 2015;198:95–101. - PubMed
-
- Findlay M, MacIsaac R, MacLeod MJ, et al. . Renal replacement modality and stroke risk in end-stage renal disease-a national registry study. Nephrol Dial Transplant. 2018;33:1564–1571. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous