

Progression to type 2 diabetes mellitus and associated risk factors after hyperglycemia first detected in pregnancy: A cross-sectional study in Cape Town, South Africa
- PMID: 31498800
- PMCID: PMC6733438
- DOI: 10.1371/journal.pmed.1002865
Progression to type 2 diabetes mellitus and associated risk factors after hyperglycemia first detected in pregnancy: A cross-sectional study in Cape Town, South Africa
Abstract
Background: Global data indicate that women with a history of hyperglycemia first detected in pregnancy (HFDP) are at up to 7 times risk of progressing to type 2 diabetes mellitus (T2DM) compared with their counterparts who have pregnancies that are not complicated by hyperglycemia. However, there are no data from the sub-Saharan African region, which has the highest projected rise in diabetes prevalence globally. The aim of this study was to determine the proportion of women who progress to T2DM and associated risk factors 5 to 6 years after HFDP in Cape Town, South Africa.
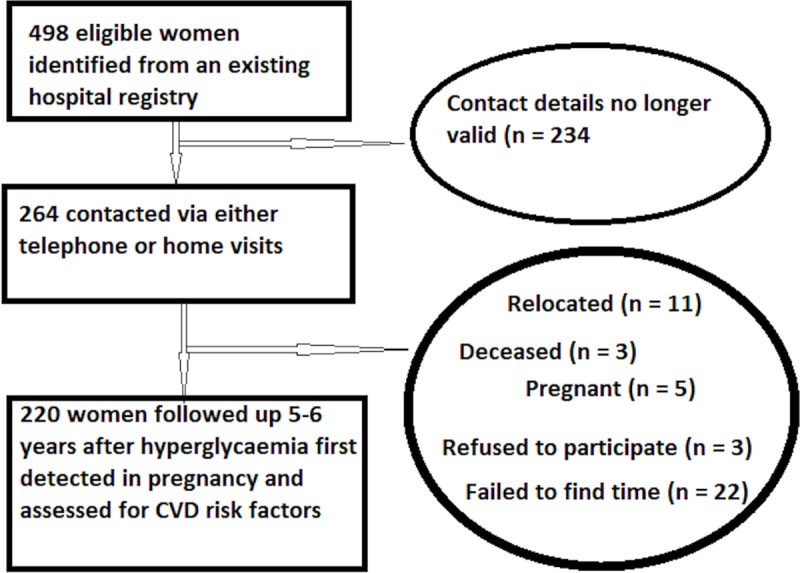
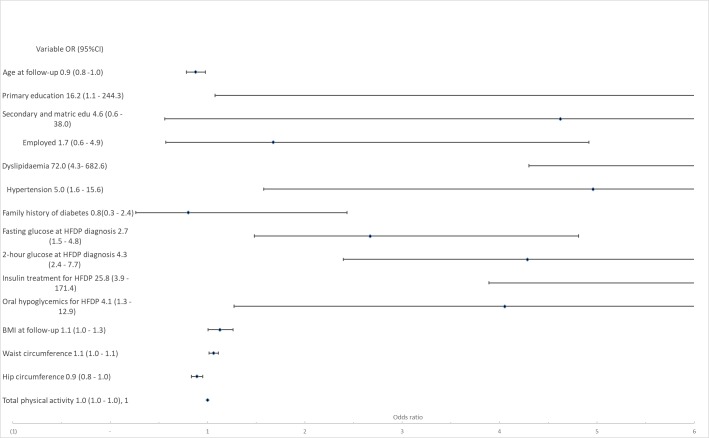
Methods and findings: All women with HFDP, at a major referral hospital in Cape Town, were followed up 5 to 6 years later using a cross-sectional study. Each participant had a 75 g oral glucose tolerance test; anthropometric measurements and a survey were administered. A total of 220 participants were followed up. At this time, their mean age was 37.2 years (SD 6.0). Forty-eight percent (95% CI 41.2-54.4) progressed to T2DM, 5.5% (95% CI 3.1-9.4) had impaired fasting glucose, and 10.5% (95% CI 7.0-15.3) had impaired glucose tolerance. Of the participants who progressed to T2DM, 47% were unaware of their diabetes status. When HFDP was categorized post hoc according to WHO 2013 guidelines, progression in the diabetes in pregnancy (DIP) group was 81% (95% CI 70.2-89.0) and 31.3% (95% CI 24.4-39.3) in the gestational diabetes mellitus (GDM) category. Factors associated with risk of progression to T2DM were; at follow-up: waist circumference (odds ratios [OR] 1.1, 95% CI 1.0-1.1, p = 0.007), hip circumference (OR 0.9, 95% CI 0.8-1.0, p = 0.001), and BMI (OR 1.1, 95% CI 1.0-1.3, p = 0.001), and at baseline: insulin (OR 25.8, 95% CI 3.9-171.4, p = 0.001) and oral hypoglycaemic treatment during HFDP (OR 4.1, 95% CI 1.3-12.9, p = 0.018), fasting (OR 2.7, 95% CI 1.5-4.8, p = 0.001), and oral glucose tolerance test 2-hour glucose concentration at HFDP diagnosis (OR 4.3, 95% CI 2.4-7.7, p < 0.001). Our findings have limitations in that we did not include a control group of women without a history of HFDP.
Conclusions: The progression to T2DM in women with previous HFDP found in this study highlights the need for interventions to delay or prevent progression to T2DM after HFDP. In addition, interventions to prevent HFDP may also contribute to reducing the risk of T2DM.
Conflict of interest statement
Authors declare no competing interests.
Figures

Similar articles
-
Cardiometabolic outcomes of women exposed to hyperglycaemia first detected in pregnancy at 3-6 years post-partum in an urban South African setting.PLoS One. 2022 Feb 9;17(2):e0263529. doi: 10.1371/journal.pone.0263529. eCollection 2022. PLoS One. 2022. PMID: 35139085 Free PMC article.
-
High prevalence of cardiovascular risk factors and insulin resistance 6 years after hyperglycemia first detected in pregnancy in Cape Town, South Africa.BMJ Open Diabetes Res Care. 2019 Nov 27;7(1):e000740. doi: 10.1136/bmjdrc-2019-000740. eCollection 2019. BMJ Open Diabetes Res Care. 2019. PMID: 31803480 Free PMC article.
-
Utility of in-hospital post-delivery fasting plasma glucose to predict postpartum glucose status in women with hyperglycaemia first detected in pregnancy: A prospective cohort study.PLoS One. 2020 Oct 5;15(10):e0239720. doi: 10.1371/journal.pone.0239720. eCollection 2020. PLoS One. 2020. PMID: 33017436 Free PMC article.
-
Hyperglycemia First Detected in Pregnancy in South Africa: Facts, Gaps, and Opportunities.Front Clin Diabetes Healthc. 2022 May 24;3:895743. doi: 10.3389/fcdhc.2022.895743. eCollection 2022. Front Clin Diabetes Healthc. 2022. PMID: 36992779 Free PMC article. Review.
-
Prevalence and risk factors for type 2 diabetes mellitus in women with gestational diabetes mellitus: a systematic review and meta-analysis.Front Endocrinol (Lausanne). 2024 Dec 23;15:1486861. doi: 10.3389/fendo.2024.1486861. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39764256 Free PMC article.
Cited by
-
Sweet Spot Regulation of Maternal Metabolic Health and Nutrition on β-Cell Mass in the Offspring.Adv Anat Embryol Cell Biol. 2024;239:157-197. doi: 10.1007/978-3-031-62232-8_7. Adv Anat Embryol Cell Biol. 2024. PMID: 39283486 Review.
-
Cardiometabolic Risk Factors in Pregnancy and Implications for Long-Term Health: Identifying the Research Priorities for Low-Resource Settings.Front Cardiovasc Med. 2020 Mar 20;7:40. doi: 10.3389/fcvm.2020.00040. eCollection 2020. Front Cardiovasc Med. 2020. PMID: 32266293 Free PMC article. Review.
-
Type 2 diabetes prevalence, awareness, and risk factors in rural Mali: a cross-sectional study.Sci Rep. 2023 Mar 6;13(1):3718. doi: 10.1038/s41598-023-29743-1. Sci Rep. 2023. PMID: 36878951 Free PMC article.
-
Increasing trend in the prevalence of gestational diabetes mellitus in Taiwan.J Diabetes Investig. 2021 Nov;12(11):2080-2088. doi: 10.1111/jdi.13595. Epub 2021 Jun 19. J Diabetes Investig. 2021. PMID: 34008344 Free PMC article.
-
Cardiometabolic outcomes of women exposed to hyperglycaemia first detected in pregnancy at 3-6 years post-partum in an urban South African setting.PLoS One. 2022 Feb 9;17(2):e0263529. doi: 10.1371/journal.pone.0263529. eCollection 2022. PLoS One. 2022. PMID: 35139085 Free PMC article.
References
-
- Rahelic D. 7th Edition of Idf Diabetes Atlas—Call for Immediate Action. Lijecnicki vjesnik. 2016;138(1–2):57–8. - PubMed
-
- Statistics South Africa. P0309.3—Mortality and causes of death in South Africa: Findings from death notification, 2016. 2018.
-
- Department of Health South Africa. World Obesity Day 2016. 2016. Available from: http://www.health.gov.za/index.php/gf-tb-program/323-world-obesity-day-2016. [cited 2019 January 30].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
