

Changing the conversation: applying a health equity framework to maternal mortality reviews
- PMID: 31499056
- PMCID: PMC11003448
- DOI: 10.1016/j.ajog.2019.08.057
Changing the conversation: applying a health equity framework to maternal mortality reviews
Abstract
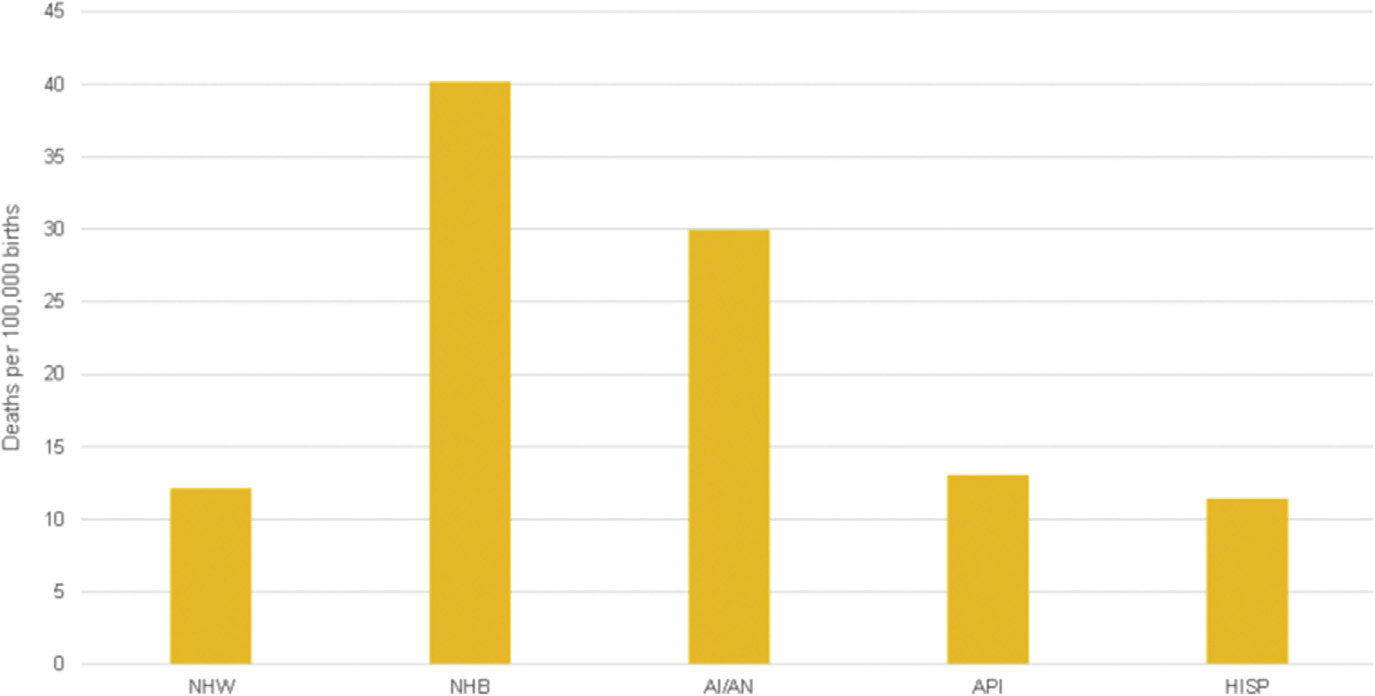
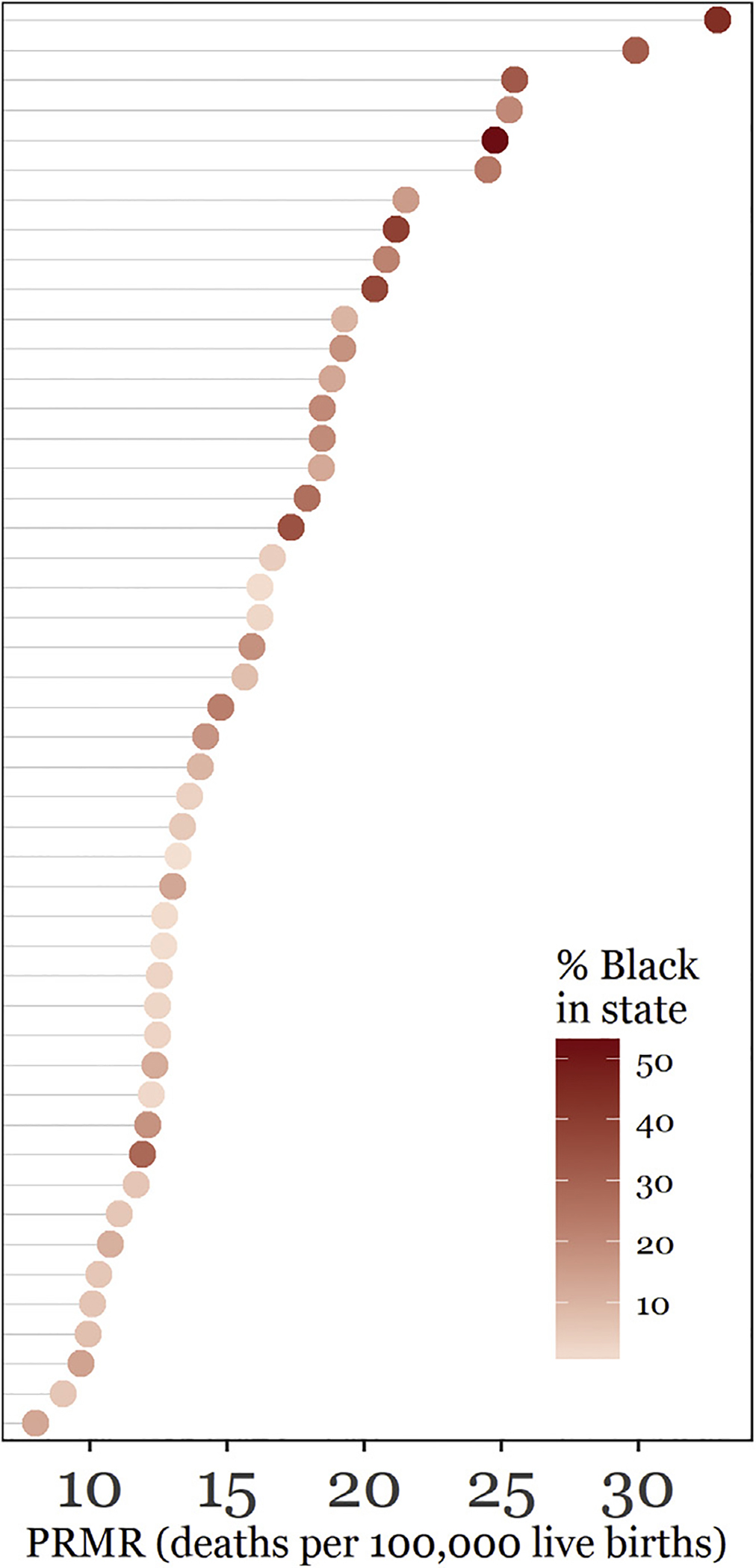
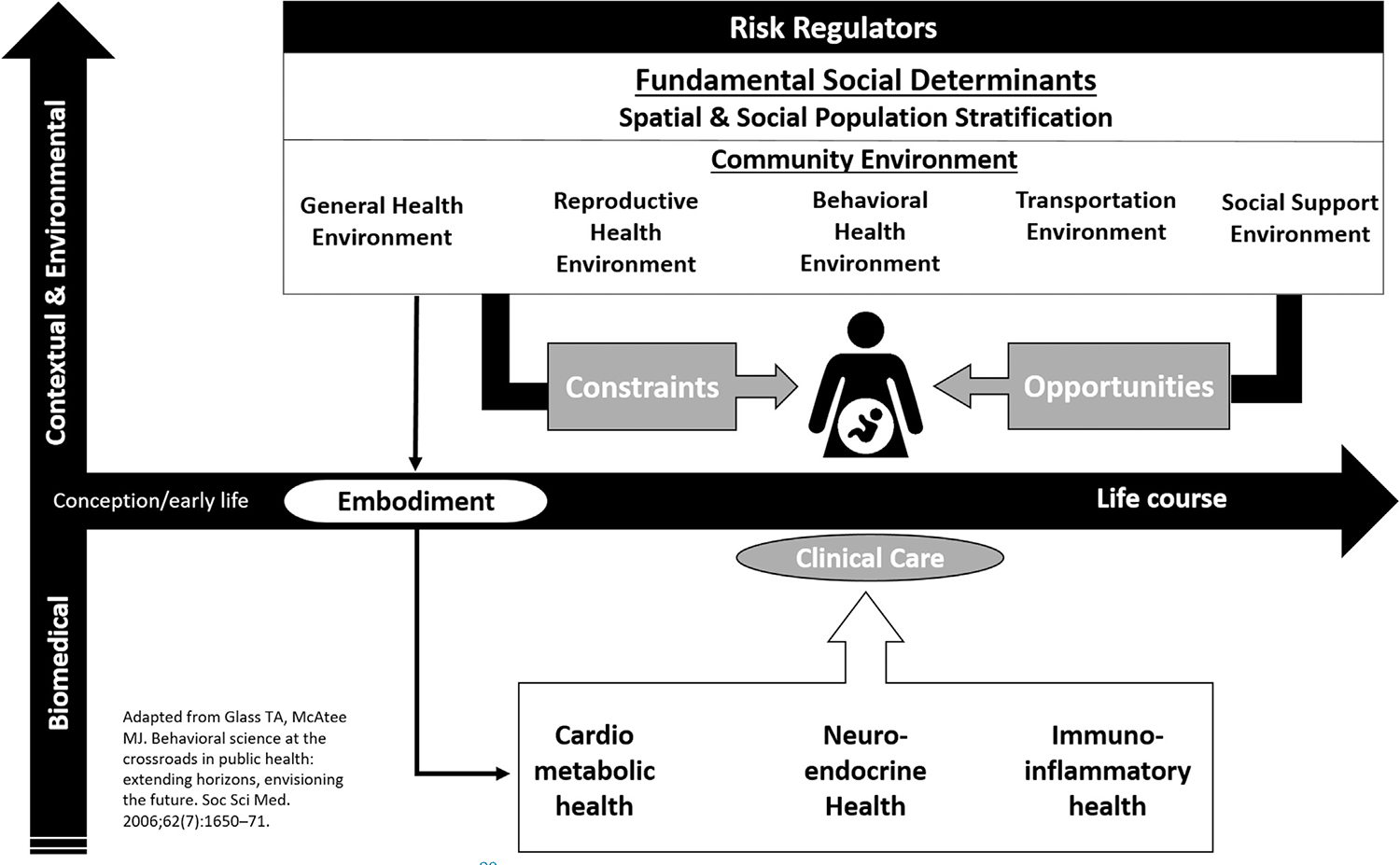
The risk of maternal death in the United States is higher than peer nations and is rising and varies dramatically by the race and place of residence of the woman. Critical efforts to reduce maternal mortality include patient risk stratification and system-level quality improvement efforts targeting specific aspects of clinical care. These efforts are important for addressing the causes of an individual's risk, but research to date suggests that individual risk factors alone do not adequately explain between-group disparities in pregnancy-related death by race, ethnicity, or geography. The holistic review and multidisciplinary makeup of maternal mortality review committees make them well positioned to fill knowledge gaps about the drivers of racial and geographic inequity in maternal death. However, committees may lack the conceptual framework, contextual data, and evidence base needed to identify community-based contributing factors to death and, when appropriate, to make recommendations for future action. By incorporating a multileveled, theory-grounded framework for causes of health inequity, along with indicators of the community vital signs, the social and community context in which women live, work, and seek health care, maternal mortality review committees may identify novel underlying factors at the community level that enhance understanding of racial and geographic inequity in maternal mortality. By considering evidence-informed community and regional resources and policies for addressing these factors, novel prevention recommendations, including recommendations that extend outside the realm of the formal health care system, may emerge.
Keywords: maternal death; maternal mortality; maternal mortality review committees; quality improvement.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- Division of Reproductive Health. Pregnancy Mortality Surveillance System [Internet]. National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention. 2017. Available at: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html. Accessed January 1, 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
