

Bone Metastases in Neuroendocrine Neoplasms: From Pathogenesis to Clinical Management
- PMID: 31500357
- PMCID: PMC6770134
- DOI: 10.3390/cancers11091332
Bone Metastases in Neuroendocrine Neoplasms: From Pathogenesis to Clinical Management
Abstract
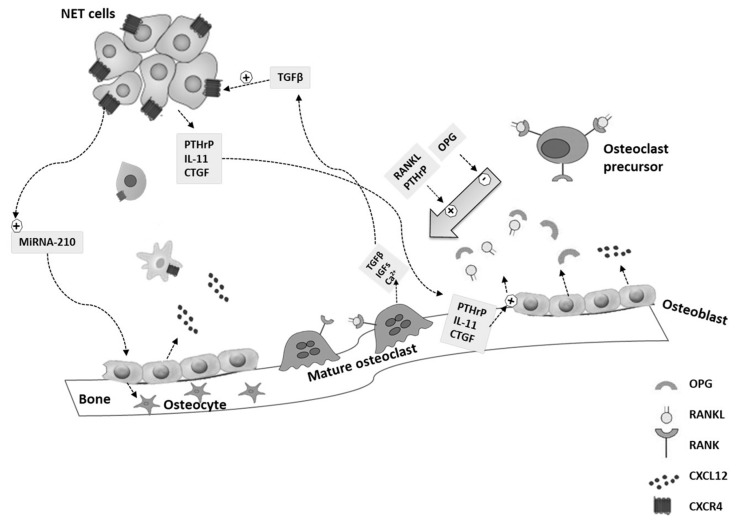
Bone represents a common site of metastases for several solid tumors. However, the ability of neuroendocrine neoplasms (NENs) to localize to bone has always been considered a rare and late event. Thanks to the improvement of therapeutic options, which results in longer survival, and of imaging techniques, particularly after the introduction of positron emission tomography (PET) with gallium peptides, the diagnosis of bone metastases (BMs) in NENs is increasing. The onset of BMs can be associated with severe skeletal complications that impair the patient's quality of life. Moreover, BMs negatively affect the prognosis of NEN patients, bringing out the lack of curative treatment options for advanced NENs. The current knowledge on BMs in gastro-entero-pancreatic (GEP) and bronchopulmonary (BP) NENs is still scant and is derived from a few retrospective studies and case reports. This review aims to perform a critical analysis of the evidence regarding the role of BMs in GEP- and BP-NENs, focusing on the molecular mechanisms underlining the development of BMs, as well as clinical presentation, diagnosis, and treatment of BMs, in an attempt to provide suggestions that can be used in clinical practice.
Keywords: bone metastases; bone microenvironment; denosumab; epithelial-to-mesenchymal transition; microRNA; neuroendocrine neoplasms; prognosis; skeletal-related events; treatment.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Faggiano A., Ferolla P., Grimaldi F., Campana D., Manzoni M., Davi M.V., Bianchi A., Valcavi R., Papini E., Giuffrida D., et al. Natural history of gastro-entero-pancreatic and thoracic neuroendocrine tumors. Data from a large prospective and retrospective Italian epidemiological study: The NET management study. J. Endocrinol. Invest. 2012;35:817–823. doi: 10.3275/8102. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
