

Validation of the Tricuspid Annular Plane Systolic Excursion/Systolic Pulmonary Artery Pressure Ratio for the Assessment of Right Ventricular-Arterial Coupling in Severe Pulmonary Hypertension
- PMID: 31500448
- PMCID: PMC7099862
- DOI: 10.1161/CIRCIMAGING.119.009047
Validation of the Tricuspid Annular Plane Systolic Excursion/Systolic Pulmonary Artery Pressure Ratio for the Assessment of Right Ventricular-Arterial Coupling in Severe Pulmonary Hypertension
Abstract
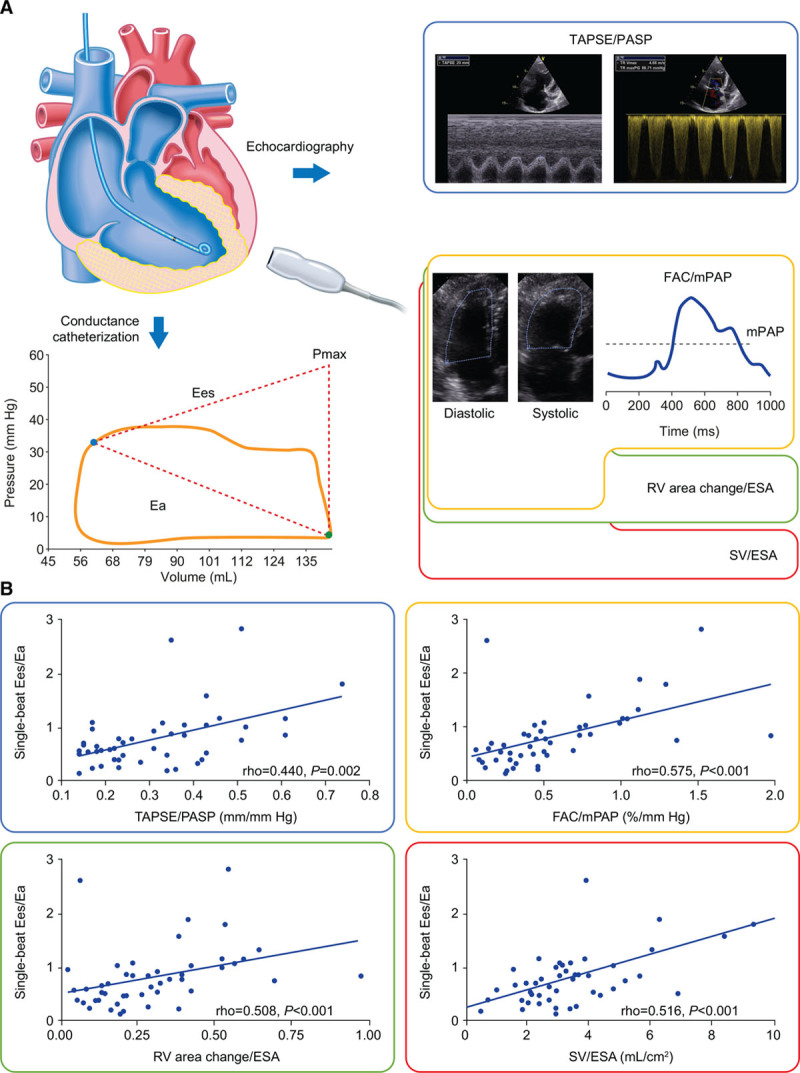
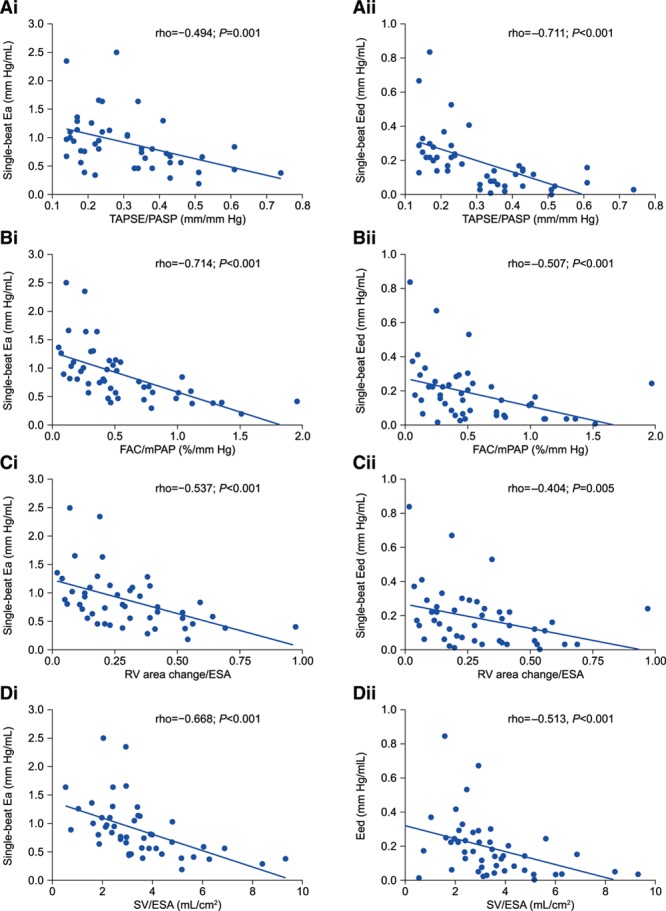
Background: The ratios of tricuspid annular plane systolic excursion (TAPSE)/echocardiographically measured systolic pulmonary artery pressure (PASP), fractional area change/invasively measured mean pulmonary artery pressure, right ventricular (RV) area change/end-systolic area, TAPSE/pulmonary artery acceleration time, and stroke volume/end-systolic area have been proposed as surrogates of RV-arterial coupling. The relationship of these surrogates with the gold standard measure of RV-arterial coupling (invasive pressure-volume loop-derived end-systolic/arterial elastance [Ees/Ea] ratio) and RV diastolic stiffness (end-diastolic elastance) in pulmonary hypertension remains incompletely understood. We evaluated the relationship of these surrogates with invasive pressure-volume loop-derived Ees/Ea and end-diastolic elastance in pulmonary hypertension.
Methods: We performed right heart echocardiography and cardiac magnetic resonance imaging 1 day before invasive measurement of pulmonary hemodynamics and single-beat RV pressure-volume loops in 52 patients with pulmonary arterial hypertension or chronic thromboembolic pulmonary hypertension. The relationships of the proposed surrogates with Ees/Ea and end-diastolic elastance were evaluated by Spearman correlation, multivariate logistic regression, and receiver operating characteristic analyses. Associations with prognosis were evaluated by Kaplan-Meier analysis.
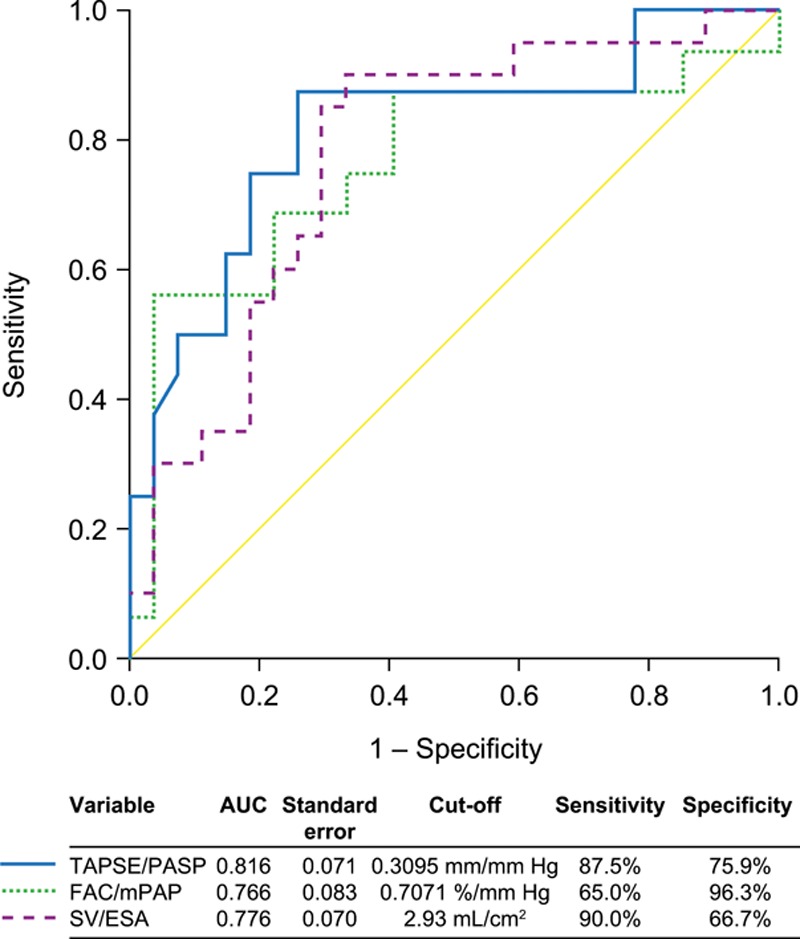
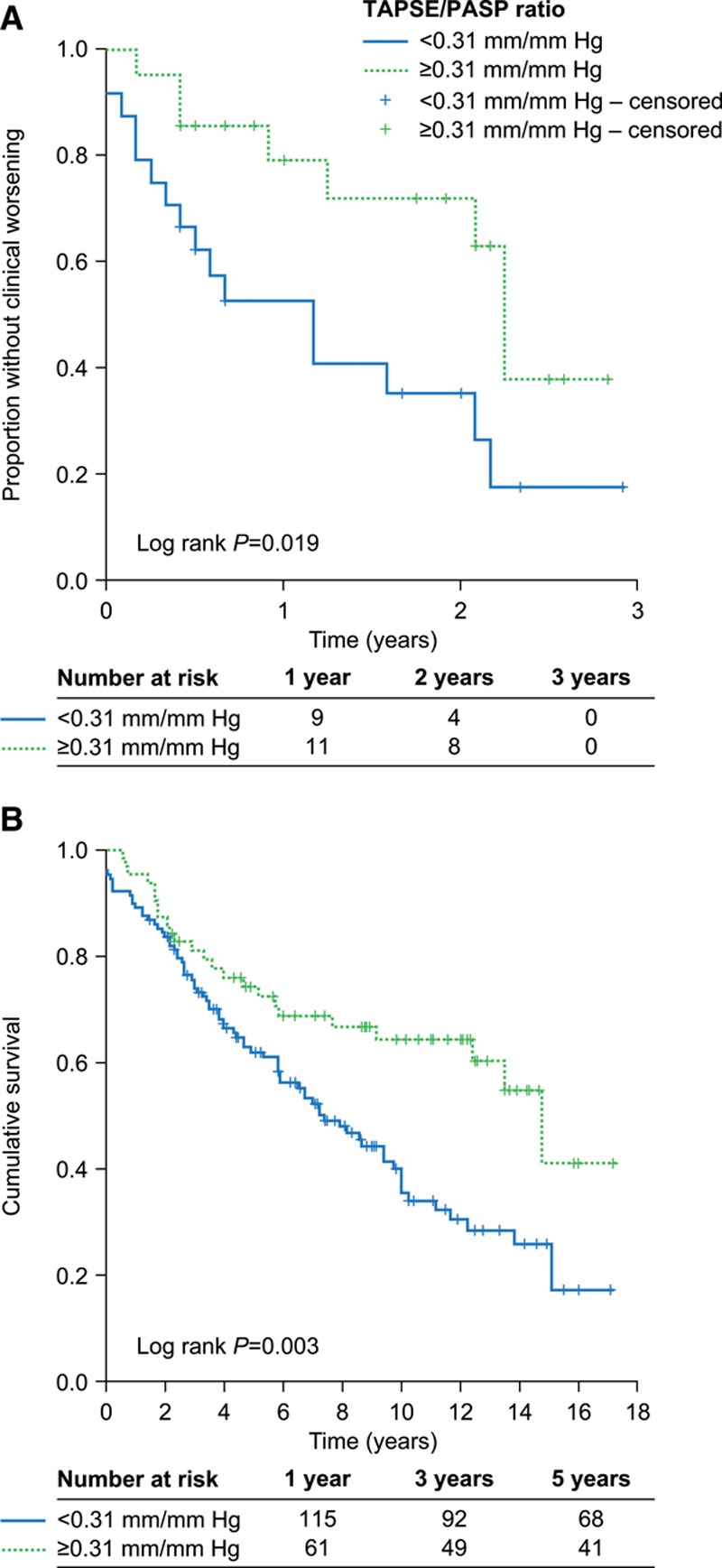
Results: TAPSE/PASP, fractional area change/mean pulmonary artery pressure, RV area change/end-systolic area, and stroke volume/end-systolic area but not TAPSE/pulmonary artery acceleration time were correlated with Ees/Ea and end-diastolic elastance. Of the surrogates, only TAPSE/PASP emerged as an independent predictor of Ees/Ea (multivariate odds ratio: 18.6; 95% CI, 0.8-96.1; P=0.08). In receiver operating characteristic analysis, a TAPSE/PASP cutoff of 0.31 mm/mm Hg (sensitivity: 87.5% and specificity: 75.9%) discriminated RV-arterial uncoupling (Ees/Ea <0.805). Patients with TAPSE/PASP <0.31 mm/mm Hg had a significantly worse prognosis than those with higher TAPSE/PASP.
Conclusions: Echocardiographically determined TAPSE/PASP is a straightforward noninvasive measure of RV-arterial coupling and is affected by RV diastolic stiffness in severe pulmonary hypertension.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT03403868.
Keywords: acceleration; echocardiography; hypertension; magnetic resonance imaging; pressure.
Figures

Comment in
-
Use of Tricuspid Annular Plane Systolic Excursion/Pulmonary Artery Systolic Pressure As a Non-Invasive Method to Assess Right Ventricular-PA Coupling in Patients With Pulmonary Hypertension.Circ Cardiovasc Imaging. 2019 Sep;12(9):e009648. doi: 10.1161/CIRCIMAGING.119.009648. Epub 2019 Sep 10. Circ Cardiovasc Imaging. 2019. PMID: 31500450 Free PMC article. No abstract available.
-
Response by Tello et al to Letter Regarding Article, "Validation of the Tricuspid Annular Plane Systolic Excursion/Systolic Pulmonary Artery Pressure Ratio for the Assessment of Right Ventricular-Arterial Coupling in Severe Pulmonary Hypertension".Circ Cardiovasc Imaging. 2019 Nov;12(11):e010059. doi: 10.1161/CIRCIMAGING.119.010059. Epub 2019 Nov 13. Circ Cardiovasc Imaging. 2019. PMID: 31718275 No abstract available.
-
Letter by Mehmood Regarding Article, "Validation of the Tricuspid Annular Plane Systolic Excursion/Systolic Pulmonary Artery Pressure Ratio for the Assessment of Right Ventricular-Arterial Coupling in Severe Pulmonary Hypertension".Circ Cardiovasc Imaging. 2019 Nov;12(11):e010002. doi: 10.1161/CIRCIMAGING.119.010002. Epub 2019 Nov 13. Circ Cardiovasc Imaging. 2019. PMID: 31718276 No abstract available.
References
-
- Lahm T, Douglas IS, Archer SL, Bogaard HJ, Chesler NC, Haddad F, Hemnes AR, Kawut SM, Kline JA, Kolb TM, Mathai SC, Mercier O, Michelakis ED, Naeije R, Tuder RM, Ventetuolo CE, Vieillard-Baron A, Voelkel NF, Vonk-Noordegraaf A, Hassoun PM; American Thoracic Society Assembly on Pulmonary Circulation. Assessment of right ventricular function in the research setting: knowledge gaps and pathways forward. an official american thoracic society research statement. Am J Respir Crit Care Med. 2018;198:e15–e43. doi: 10.1164/rccm.201806-1160ST - PMC - PubMed
-
- Vonk Noordegraaf A, Chin KM, Haddad F, Hassoun PM, Hemnes AR, Hopkins SR, Kawut SM, Langleben D, Lumens J, Naeije R. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: an update. Eur Respir J. 2019;53:1801900 doi: 10.1183/13993003.01900-2018 - PMC - PubMed
-
- Vonk Noordegraaf A, Westerhof BE, Westerhof N. The relationship between the right ventricle and its load in pulmonary hypertension. J Am Coll Cardiol. 2017;69:236–243. doi: 10.1016/j.jacc.2016.10.047 - PubMed
-
- Tello K, Dalmer A, Axmann J, Vanderpool R, Ghofrani HA, Naeije R, Roller F, Seeger W, Sommer N, Wilhelm J, Gall H, Richter MJ. Reserve of right ventricular-arterial coupling in the setting of chronic overload. Circ Heart Fail. 2019;12:e005512 doi: 10.1161/CIRCHEARTFAILURE.118.005512 - PubMed
-
- Guazzi M, Bandera F, Pelissero G, Castelvecchio S, Menicanti L, Ghio S, Temporelli PL, Arena R. Tricuspid annular plane systolic excursion and pulmonary arterial systolic pressure relationship in heart failure: an index of right ventricular contractile function and prognosis. Am J Physiol Heart Circ Physiol. 2013;305:H1373–H1381. doi: 10.1152/ajpheart.00157.2013 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
