

Effect of remote ischaemic conditioning on clinical outcomes in patients with acute myocardial infarction (CONDI-2/ERIC-PPCI): a single-blind randomised controlled trial
- PMID: 31500849
- PMCID: PMC6891239
- DOI: 10.1016/S0140-6736(19)32039-2
Effect of remote ischaemic conditioning on clinical outcomes in patients with acute myocardial infarction (CONDI-2/ERIC-PPCI): a single-blind randomised controlled trial
Abstract
Background: Remote ischaemic conditioning with transient ischaemia and reperfusion applied to the arm has been shown to reduce myocardial infarct size in patients with ST-elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PPCI). We investigated whether remote ischaemic conditioning could reduce the incidence of cardiac death and hospitalisation for heart failure at 12 months.
Methods: We did an international investigator-initiated, prospective, single-blind, randomised controlled trial (CONDI-2/ERIC-PPCI) at 33 centres across the UK, Denmark, Spain, and Serbia. Patients (age >18 years) with suspected STEMI and who were eligible for PPCI were randomly allocated (1:1, stratified by centre with a permuted block method) to receive standard treatment (including a sham simulated remote ischaemic conditioning intervention at UK sites only) or remote ischaemic conditioning treatment (intermittent ischaemia and reperfusion applied to the arm through four cycles of 5-min inflation and 5-min deflation of an automated cuff device) before PPCI. Investigators responsible for data collection and outcome assessment were masked to treatment allocation. The primary combined endpoint was cardiac death or hospitalisation for heart failure at 12 months in the intention-to-treat population. This trial is registered with ClinicalTrials.gov (NCT02342522) and is completed.
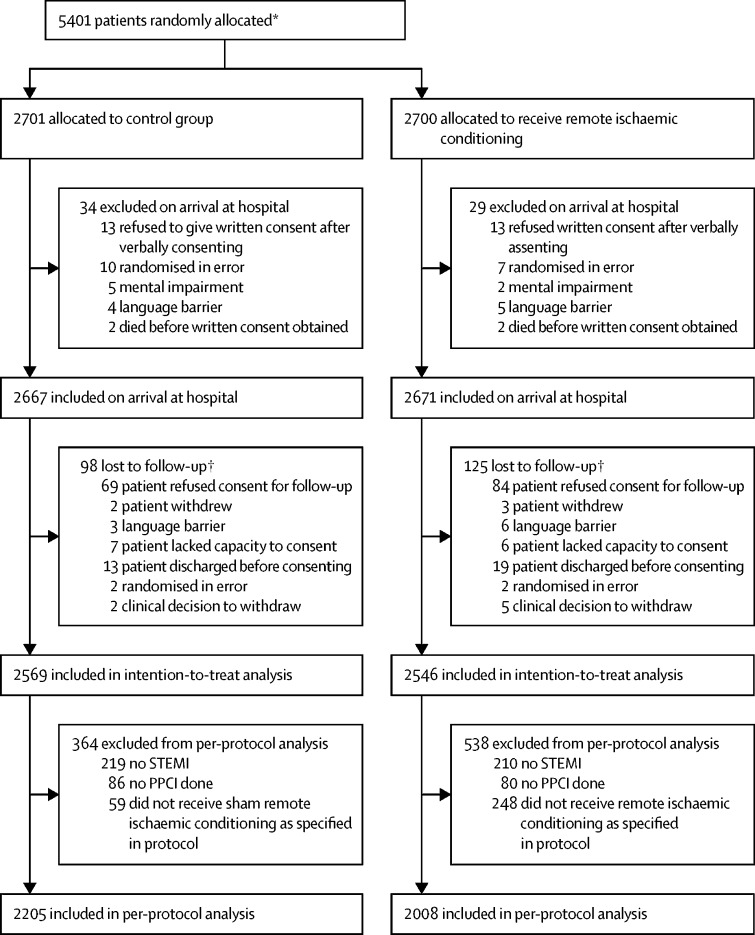
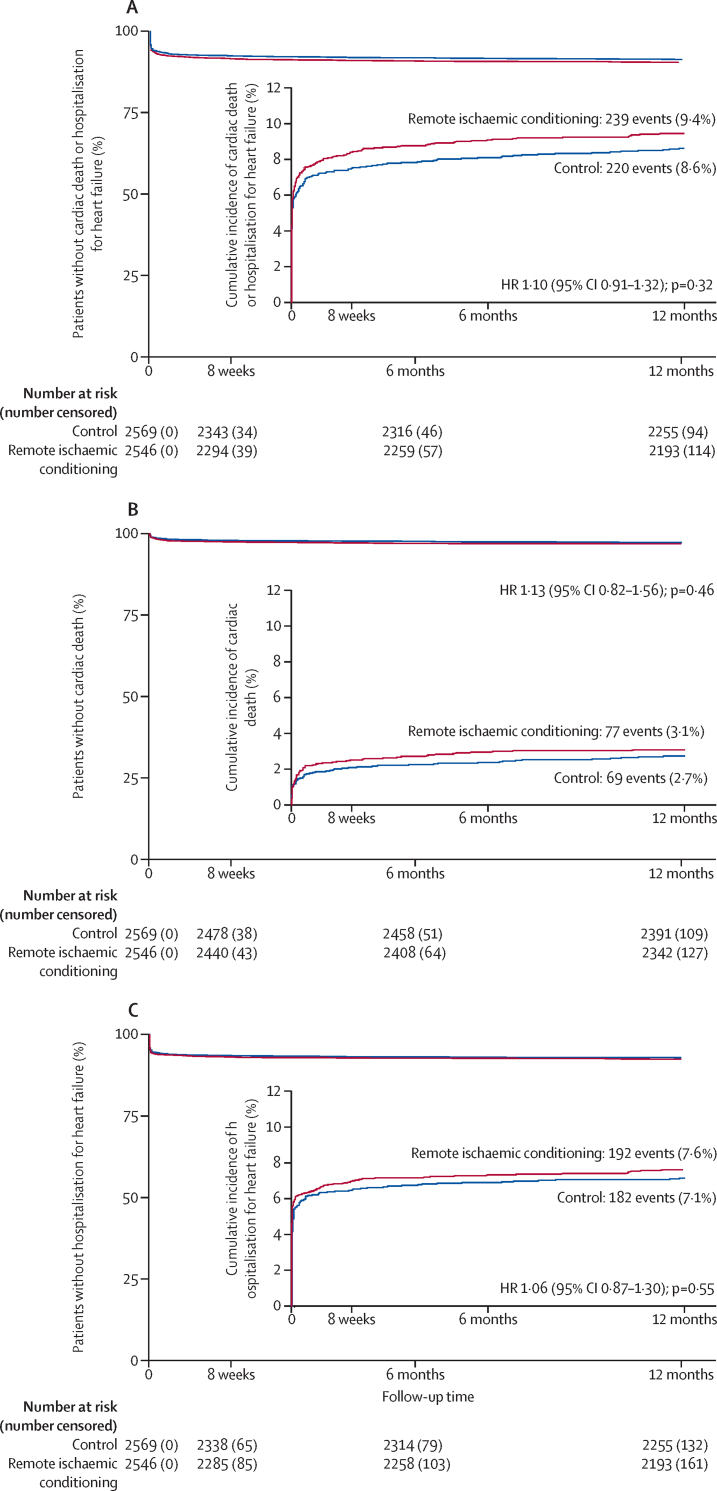
Findings: Between Nov 6, 2013, and March 31, 2018, 5401 patients were randomly allocated to either the control group (n=2701) or the remote ischaemic conditioning group (n=2700). After exclusion of patients upon hospital arrival or loss to follow-up, 2569 patients in the control group and 2546 in the intervention group were included in the intention-to-treat analysis. At 12 months post-PPCI, the Kaplan-Meier-estimated frequencies of cardiac death or hospitalisation for heart failure (the primary endpoint) were 220 (8·6%) patients in the control group and 239 (9·4%) in the remote ischaemic conditioning group (hazard ratio 1·10 [95% CI 0·91-1·32], p=0·32 for intervention versus control). No important unexpected adverse events or side effects of remote ischaemic conditioning were observed.
Interpretation: Remote ischaemic conditioning does not improve clinical outcomes (cardiac death or hospitalisation for heart failure) at 12 months in patients with STEMI undergoing PPCI.
Funding: British Heart Foundation, University College London Hospitals/University College London Biomedical Research Centre, Danish Innovation Foundation, Novo Nordisk Foundation, TrygFonden.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
The broken promise of remote ischaemic conditioning.Lancet. 2019 Oct 19;394(10207):1389-1390. doi: 10.1016/S0140-6736(19)32047-1. Epub 2019 Sep 6. Lancet. 2019. PMID: 31500850 No abstract available.
-
Remote Ischemic Conditioning in Acute Myocardial Infarction - Implications of the CONDI-2/ERIC-PPCI Trial for Prehospital and Emergency Medicine.Prehosp Emerg Care. 2020 Nov-Dec;24(6):862-864. doi: 10.1080/10903127.2019.1704324. Epub 2020 Jan 27. Prehosp Emerg Care. 2020. PMID: 31986074
References
-
- Schmidt MR, Smerup M, Konstantinov IE. Intermittent peripheral tissue ischemia during coronary ischemia reduces myocardial infarction through a KATP-dependent mechanism: first demonstration of remote ischemic perconditioning. Am J Physiol Heart Circ Physiol. 2007;292:H1883–H1890. - PubMed
-
- Kharbanda RK, Mortensen UM, White PA. Transient limb ischemia induces remote ischemic preconditioning in vivo. Circulation. 2002;106:2881–2883. - PubMed
-
- Bøtker HE, Kharbanda R, Schmidt MR. Remote ischaemic conditioning before hospital admission, as a complement to angioplasty, and effect on myocardial salvage in patients with acute myocardial infarction: a randomised trial. Lancet. 2010;375:727–734. - PubMed
