

Defining Dysbiosis for a Cluster of Chronic Diseases
- PMID: 31501492
- PMCID: PMC6733864
- DOI: 10.1038/s41598-019-49452-y
Defining Dysbiosis for a Cluster of Chronic Diseases
Abstract
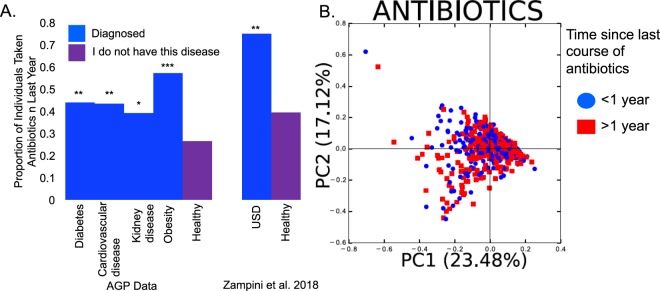
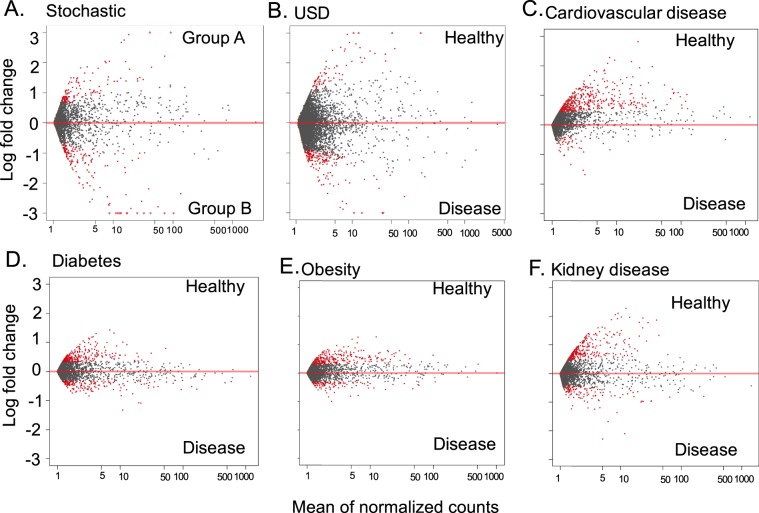
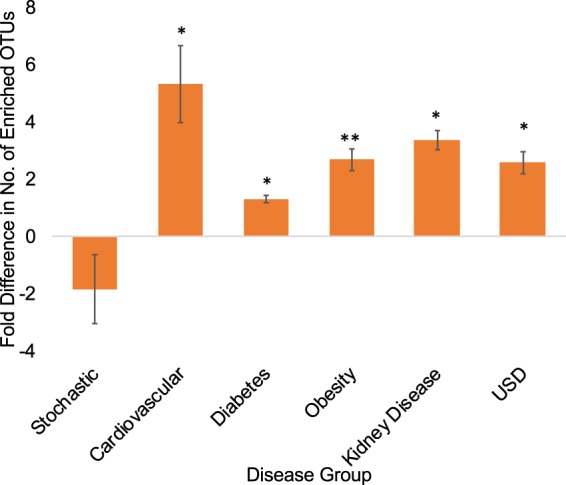
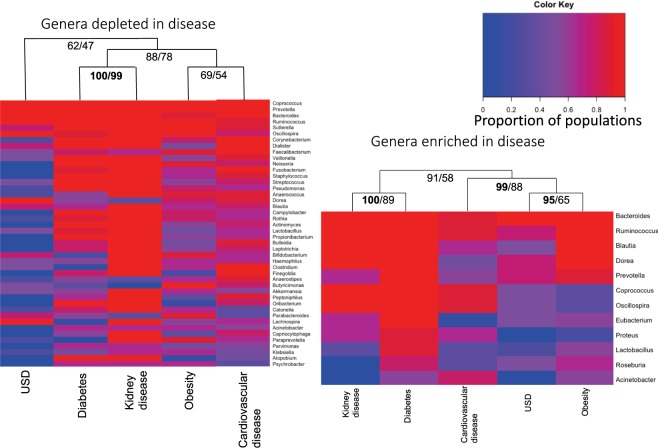
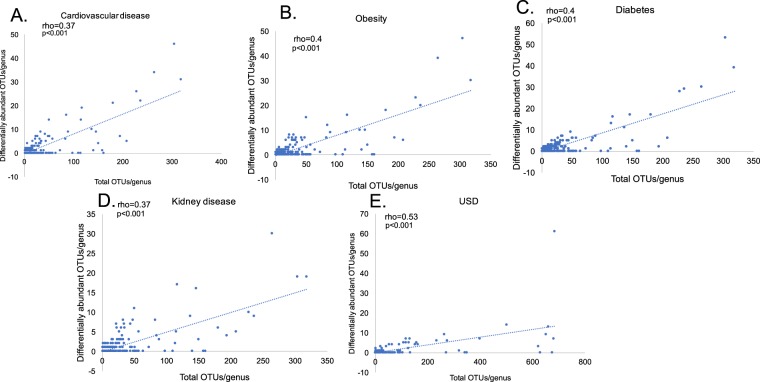
The prevalence of many chronic diseases has increased over the last decades. It has been postulated that dysbiosis driven by environmental factors such as antibiotic use is shifting the microbiome in ways that increase inflammation and the onset of chronic disease. Dysbiosis can be defined through the loss or gain of bacteria that either promote health or disease, respectively. Here we use multiple independent datasets to determine the nature of dysbiosis for a cluster of chronic diseases that includes urinary stone disease (USD), obesity, diabetes, cardiovascular disease, and kidney disease, which often exist as co-morbidities. For all disease states, individuals exhibited a statistically significant association with antibiotics in the last year compared to healthy counterparts. There was also a statistically significant association between antibiotic use and gut microbiota composition. Furthermore, each disease state was associated with a loss of microbial diversity in the gut. Three genera, Bacteroides, Prevotella, and Ruminococcus, were the most common dysbiotic taxa in terms of being enriched or depleted in disease populations and was driven in part by the diversity of operational taxonomic units (OTUs) within these genera. Results of the cross-sectional analysis suggest that antibiotic-driven loss of microbial diversity may increase the risk for chronic disease. However, longitudinal studies are needed to confirm the causative effect of diversity loss for chronic disease risk.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
