

Whether the newly modified rhizotomy protocol is applicable to guide single-level approach SDR to treat spastic quadriplegia and diplegia in pediatric patients with cerebral palsy?
- PMID: 31502037
- PMCID: PMC7434794
- DOI: 10.1007/s00381-019-04368-w
Whether the newly modified rhizotomy protocol is applicable to guide single-level approach SDR to treat spastic quadriplegia and diplegia in pediatric patients with cerebral palsy?
Abstract
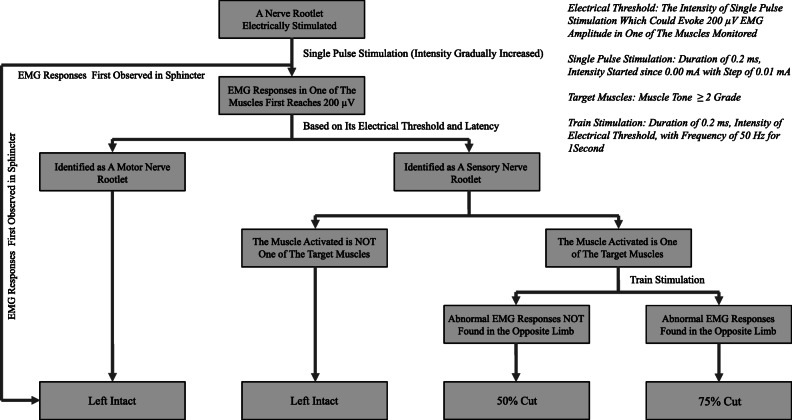
Purpose: Our aim was to test whether the newly modified rhizotomy protocol which could be effectively used to guide single-level approach selective dorsal rhizotomy (SL-SDR) to treat spastic hemiplegic cases by mainly releasing those spastic muscles (target muscles) marked pre-operatively in their lower limbs was still applicable in spastic quadriplegic or diplegic cerebral palsy (CP) cases in pediatric population.
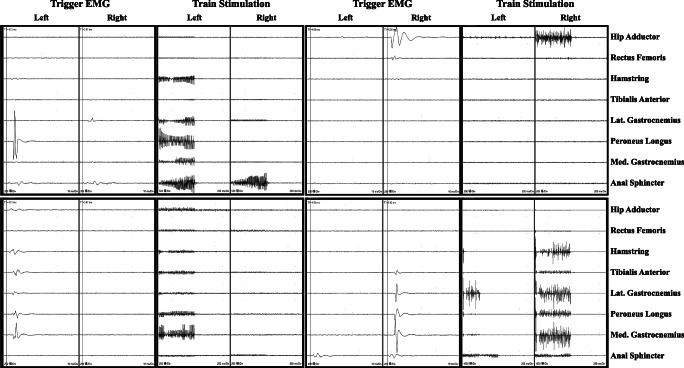
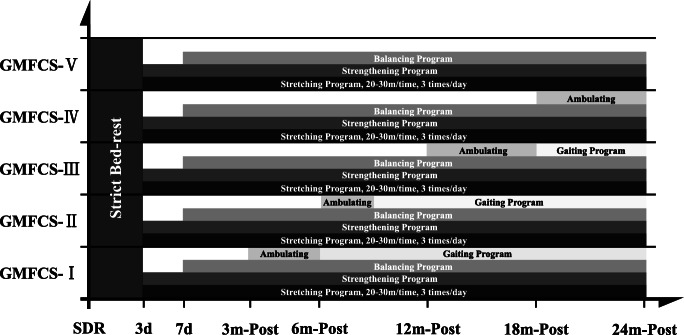
Methods: In the current study, we retrospectively conducted a cohort review of cases younger than 14 years of age diagnosed with spastic quadriplegic or diplegic CP who undergone our modified protocol-guided SL-SDR in the Department of Neurosurgery, Children's Hospital of Shanghai since July 2016 to November 2017 with at least 12 months post-op intensive rehabilitation program (pre-op GMFCS level-based). Clinical data including demographics, intra-operative EMG responses interpretation, and relevant assessment of included cases were taken from the database. Inclusion and exclusion criteria were set for the selection of patients in the current study. Muscle tone (modified Ashworth scale) and strength of those spastic muscles (muscle strength grading scale), range of motion (ROM) of those joints involved, the level of Gross Motor Function Classification System (GMFCS), and Gross Motor Function Measure 66 items (GMFM-66) score of those cases were our focus.
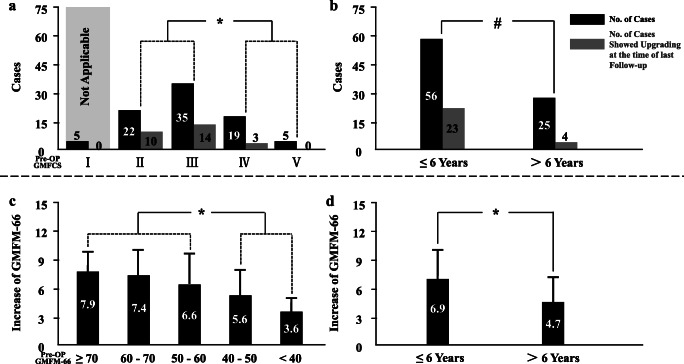
Results: A total of 86 eligible cases were included in our study (62 boys). Among these patients, 61.6% were quadriplegic. Pre-operatively, almost 2/3 of our cases were with GMFCS levels II and III. Mean age at the time of surgery in these cases was 6.2 (3.5-12) years. Pre-op assessment marked 582 target muscles in these patients. Numbers of nerve rootlets tested during SDR procedure were between 52 and 84 across our cases, with a mean of 66.5 ± 6.7/case. Among those tested (5721 in 86 cases), 47.9% (2740) were identified as lower limb-related sensory rootlets. Our protocol successfully differentiated sensory rootlets which were considered to be associated with spasticity of target muscles across all our 86 cases (ranged from 3 to 21). Based on our protocol, 871 dorsal nerve rootlets were sectioned 50%, and 78 were cut 75%. Muscle tone of those target muscles reduced significantly right after SL-SDR procedure (3 weeks post- vs. pre-op, 1.7 ± 0.5 vs. 2.6 ± 0.7). After an intensive rehabilitation program for 19.9 ± 6.0 months, muscle tone continued to decrease to 1.4 ± 0.5. With the reduction of muscle tone, strength of those target muscles in our cases improved dramatically with statistical significance achieved (3.9 ± 1.0 at the time of last follow-up vs. 3.3 ± 0.8 pre-op), and as well as ROM. Increase in GMFCS level and GMFM-66 score was observed at the time of last follow-up with a mean of 0.4 ± 0.6 and 6.1 ± 3.2, respectively, when compared with that at pre-op. In 81 cases with their pre-op GMFCS levels II to V, 27 (33.3%) presented improvement with regard to GMFCS level upgrade, among which 4 (4.9%) even upgraded over 2 levels. Better results with regard to upgrading in level of GMFCS were observed in cases with pre-op levels II and III when compared with those with levels IV and V (24/57 vs. 3/24). Upgrading percentage in cases younger than 6 years at surgery was significantly greater than in those older (23/56 vs. 4/25). Cases with their pre-op GMFM-66 score ≥ 50 had greater score increase of GMFM-66 when compared with those less (7.1 ± 3.4 vs. 5.1 ± 2.8). In the meanwhile, better score improvement was revealed in cases when SDR performed at younger age (6.9 ± 3.3 in case ≤ 6 years vs. 4.7 ± 2.7 in case > 6 years). No permanent surgery-related complications were recorded in the current study.
Conclusion: SL-SDR when guided by our newly modified rhizotomy protocol was still feasible to treat pediatric CP cases with spastic quadriplegia and diplegia. Cases in this condition could benefit from such a procedure when followed by our intensive rehabilitation program with regard to their motor function.
Keywords: Dorsal rhizotomy; Intra-operative neuroelectrophysiology; Outcome; Rootlet selection; Spastic cerebral palsy.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures
Similar articles
-
The role of intra-operative neuroelectrophysiological monitoring in single-level approach selective dorsal rhizotomy.Childs Nerv Syst. 2020 Sep;36(9):1925-1933. doi: 10.1007/s00381-019-04408-5. Epub 2019 Nov 4. Childs Nerv Syst. 2020. PMID: 31686140
-
Feasibility and effectiveness of a newly modified protocol-guided selective dorsal rhizotomy via single-level approach to treat spastic hemiplegia in pediatric cases with cerebral palsy.Childs Nerv Syst. 2019 Nov;35(11):2171-2178. doi: 10.1007/s00381-019-04194-0. Epub 2019 May 29. Childs Nerv Syst. 2019. PMID: 31144022
-
Long-term functional benefits of selective dorsal rhizotomy for spastic cerebral palsy.J Neurosurg Pediatr. 2013 Aug;12(2):142-50. doi: 10.3171/2013.4.PEDS12539. Epub 2013 May 28. J Neurosurg Pediatr. 2013. PMID: 23713680
-
Palliative single-level selective dorsal rhizotomy for children with spastic cerebral palsy Gross Motor Function Classification System level IV and V: a case series and systematic review of the literature.Neurosurg Focus. 2024 Jun;56(6):E6. doi: 10.3171/2024.3.FOCUS2478. Neurosurg Focus. 2024. PMID: 38823044
-
Selective dorsal rhizotomies in the treatment of spasticity related to cerebral palsy.Childs Nerv Syst. 2007 Sep;23(9):991-1002. doi: 10.1007/s00381-007-0398-2. Epub 2007 Jul 21. Childs Nerv Syst. 2007. PMID: 17643249 Review.
Cited by
-
Quantitative identification of ventral/dorsal nerves through intraoperative neurophysiological monitoring by supervised machine learning.Front Pediatr. 2023 May 18;11:1118924. doi: 10.3389/fped.2023.1118924. eCollection 2023. Front Pediatr. 2023. PMID: 37274819 Free PMC article.
-
Urodynamic study findings and related influential factors in pediatric spastic cerebral palsy.Sci Rep. 2022 Apr 28;12(1):6962. doi: 10.1038/s41598-022-11057-3. Sci Rep. 2022. PMID: 35484196 Free PMC article.
-
Rootlet Selection by Crescendo Single-Pulse Evoked Compound Muscle Action Potential Interpretation During Selective Dorsal Rhizotomy.Adv Tech Stand Neurosurg. 2025;51:123-138. doi: 10.1007/978-3-031-86441-4_10. Adv Tech Stand Neurosurg. 2025. PMID: 40445345
-
Enhancing understanding and optimizing outcomes: insights from selective dorsal rhizotomy in pediatric cerebral palsy.Transl Pediatr. 2024 May 31;13(5):873-874. doi: 10.21037/tp-24-106. Epub 2024 May 27. Transl Pediatr. 2024. PMID: 38840686 Free PMC article. No abstract available.
-
Modified Selective Dorsal Rhizotomy Exposure Method for Adults With Spastic Paralysis of the Lower Limbs.Oper Neurosurg. 2023 Dec 12;26(5):527-32. doi: 10.1227/ons.0000000000001011. Online ahead of print. Oper Neurosurg. 2023. PMID: 38084948 Free PMC article.
References
-
- Zhan Q, Tang L, Wang Y, Xiao B, Shen M, Jiang S, Mei R, Lyu Z (2019) Feasibility and effectiveness of a newly modified protocol-guided selective dorsal rhizotomy via single-level approach to treat spastic hemiplegia in pediatric cases with cerebral palsy. Childs Nerv Syst. 10.1007/s00381-019-04194-0 - PubMed
-
- Park TS, Johnston JM. Surgical techniques of selective dorsal rhizotomy for spastic cerebral palsy. Neurosurg Focus. 2006;21:1–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
