

Prediction of Upstaged Ductal Carcinoma In Situ Using Forced Labeling and Domain Adaptation
- PMID: 31502960
- PMCID: PMC7757748
- DOI: 10.1109/TBME.2019.2940195
Prediction of Upstaged Ductal Carcinoma In Situ Using Forced Labeling and Domain Adaptation
Abstract
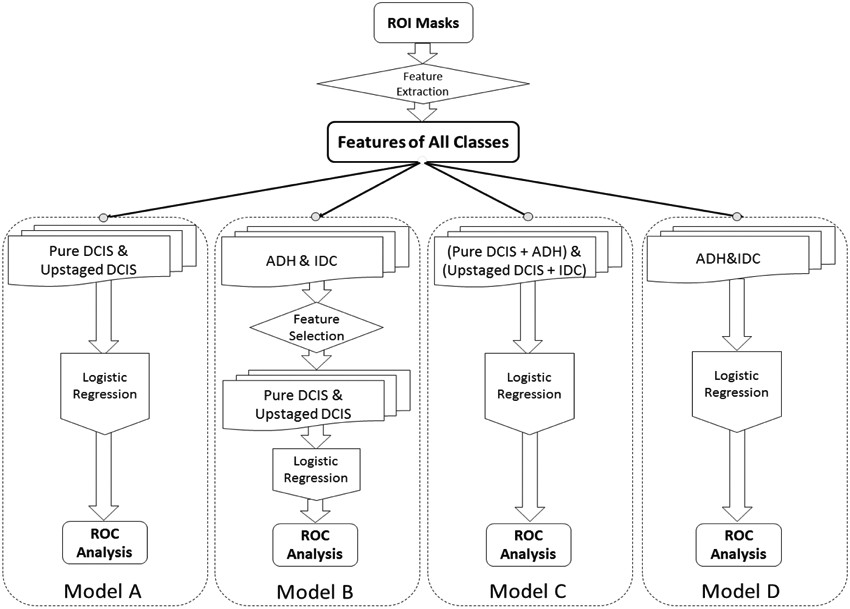
Objective: The goal of this study is to use adjunctive classes to improve a predictive model whose performance is limited by the common problems of small numbers of primary cases, high feature dimensionality, and poor class separability. Specifically, our clinical task is to use mammographic features to predict whether ductal carcinoma in situ (DCIS) identified at needle core biopsy will be later upstaged or shown to contain invasive breast cancer.
Methods: To improve the prediction of pure DCIS (negative) versus upstaged DCIS (positive) cases, this study considers the adjunctive roles of two related classes: atypical ductal hyperplasia (ADH), a non-cancer type of breast abnormity, and invasive ductal carcinoma (IDC), with 113 computer vision based mammographic features extracted from each case. To improve the baseline Model A's classification of pure vs. upstaged DCIS, we designed three different strategies (Models B, C, D) with different ways of embedding features or inputs.
Results: Based on ROC analysis, the baseline Model A performed with AUC of 0.614 (95% CI, 0.496-0.733). All three new models performed better than the baseline, with domain adaptation (Model D) performing the best with an AUC of 0.697 (95% CI, 0.595-0.797).
Conclusion: We improved the prediction performance of DCIS upstaging by embedding two related pathology classes in different training phases.
Significance: The three new strategies of embedding related class data all outperformed the baseline model, thus demonstrating not only feature similarities among these different classes, but also the potential for improving classification by using other related classes.
Figures







Similar articles
-
Mixed-Methods Study to Predict Upstaging of DCIS to Invasive Disease on Mammography.AJR Am J Roentgenol. 2021 Apr;216(4):903-911. doi: 10.2214/AJR.20.23679. Epub 2021 Feb 3. AJR Am J Roentgenol. 2021. PMID: 32783550 Free PMC article.
-
Can Occult Invasive Disease in Ductal Carcinoma In Situ Be Predicted Using Computer-extracted Mammographic Features?Acad Radiol. 2017 Sep;24(9):1139-1147. doi: 10.1016/j.acra.2017.03.013. Epub 2017 May 11. Acad Radiol. 2017. PMID: 28506510 Free PMC article.
-
Prediction of Occult Invasive Disease in Ductal Carcinoma in Situ Using Deep Learning Features.J Am Coll Radiol. 2018 Mar;15(3 Pt B):527-534. doi: 10.1016/j.jacr.2017.11.036. Epub 2018 Feb 2. J Am Coll Radiol. 2018. PMID: 29398498 Free PMC article.
-
Pathology of ductal carcinoma in situ of the breast: a heterogeneous entity in need of greater understanding.Ann Acad Med Singap. 2001 Nov;30(6):671-6; quiz 677. Ann Acad Med Singap. 2001. PMID: 11817303 Review.
-
Ductal carcinoma in situ of breast: update 2019.Pathology. 2019 Oct;51(6):563-569. doi: 10.1016/j.pathol.2019.07.005. Epub 2019 Aug 28. Pathology. 2019. PMID: 31472981 Free PMC article. Review.
Cited by
-
Anomaly Detection of Calcifications in Mammography Based on 11,000 Negative Cases.IEEE Trans Biomed Eng. 2022 May;69(5):1639-1650. doi: 10.1109/TBME.2021.3126281. Epub 2022 Apr 21. IEEE Trans Biomed Eng. 2022. PMID: 34788216 Free PMC article.
-
Predicting Underestimation of Invasive Cancer in Patients with Core-Needle-Biopsy-Diagnosed Ductal Carcinoma In Situ Using Deep Learning Algorithms.Tomography. 2022 Dec 20;9(1):1-11. doi: 10.3390/tomography9010001. Tomography. 2022. PMID: 36648988 Free PMC article.
-
Mixed-Methods Study to Predict Upstaging of DCIS to Invasive Disease on Mammography.AJR Am J Roentgenol. 2021 Apr;216(4):903-911. doi: 10.2214/AJR.20.23679. Epub 2021 Feb 3. AJR Am J Roentgenol. 2021. PMID: 32783550 Free PMC article.
-
Classification performance bias between training and test sets in a limited mammography dataset.PLoS One. 2024 Feb 7;19(2):e0282402. doi: 10.1371/journal.pone.0282402. eCollection 2024. PLoS One. 2024. PMID: 38324545 Free PMC article.
-
Prediction of Upstaging in Ductal Carcinoma in Situ Based on Mammographic Radiomic Features.Radiology. 2022 Apr;303(1):54-62. doi: 10.1148/radiol.210407. Epub 2022 Jan 4. Radiology. 2022. PMID: 34981975 Free PMC article.
References
-
- Ali SZ, Surveillance of BIRADS 3 lesions. Breast J, 2017. 23(5): p. 617. - PubMed
-
- Virnig BA, et al., Ductal carcinoma in situ of the breast: a systematic review of incidence, treatment, and outcomes. Journal of the National Cancer Institute, 2010. 102(3): p. 170–178. - PubMed
-
- Sanders ME, et al., The natural history of low-grade ductal carcinoma in situ of the breast in women treated by biopsy only revealed over 30 years of long-term follow-up. Cancer, 2005. 103(12): p. 2481–4. - PubMed
-
- Collins LC, et al., Outcome of patients with ductal carcinoma in situ untreated after diagnostic biopsy: results from the Nurses' Health Study. Cancer, 2005. 103(9): p. 1778–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
