

Leveraging a Comprehensive Program to Implement a Colorectal Surgical Site Infection Reduction Bundle in a Statewide Quality Improvement Collaborative
- PMID: 31503066
- PMCID: PMC7775039
- DOI: 10.1097/SLA.0000000000003524
Leveraging a Comprehensive Program to Implement a Colorectal Surgical Site Infection Reduction Bundle in a Statewide Quality Improvement Collaborative
Abstract
Objectives: Our objective was to examine the implementation and associated clinical outcomes of a comprehensive surgical site infection (SSI) reduction bundle in a large statewide surgical quality improvement collaborative leveraging a multifaceted implementation strategy.
Summary background data: Bundled perioperative interventions reduce colorectal SSI rates when enacted at individual hospitals, but the ability to implement comprehensive SSI bundles and to examine the resultant clinical effectiveness within a larger, diverse population of hospitals is unknown.
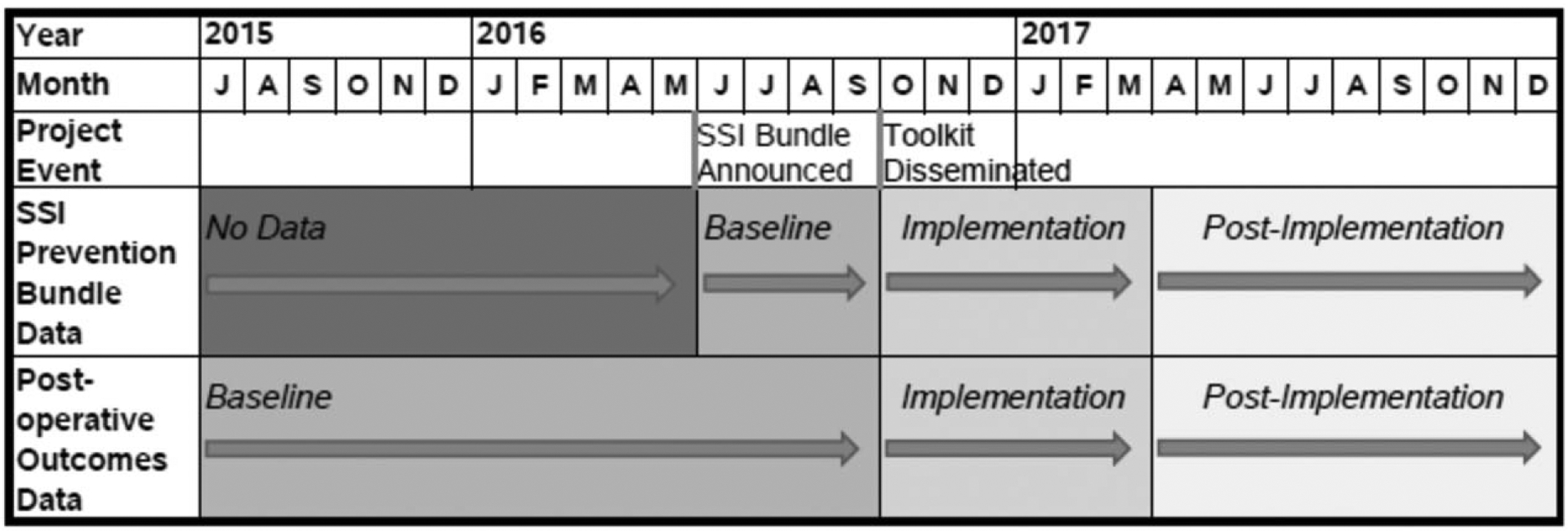
Methods: A multifaceted SSI reduction bundle was developed and implemented in a large statewide surgical quality improvement collaborative through a novel implementation program consisting of guided implementation, data feedback, mentorship, process improvement training/coaching, and targeted-implementation toolkits. Bundle adherence and ACS NSQIP outcomes were examined preimplementation versus postimplementation.
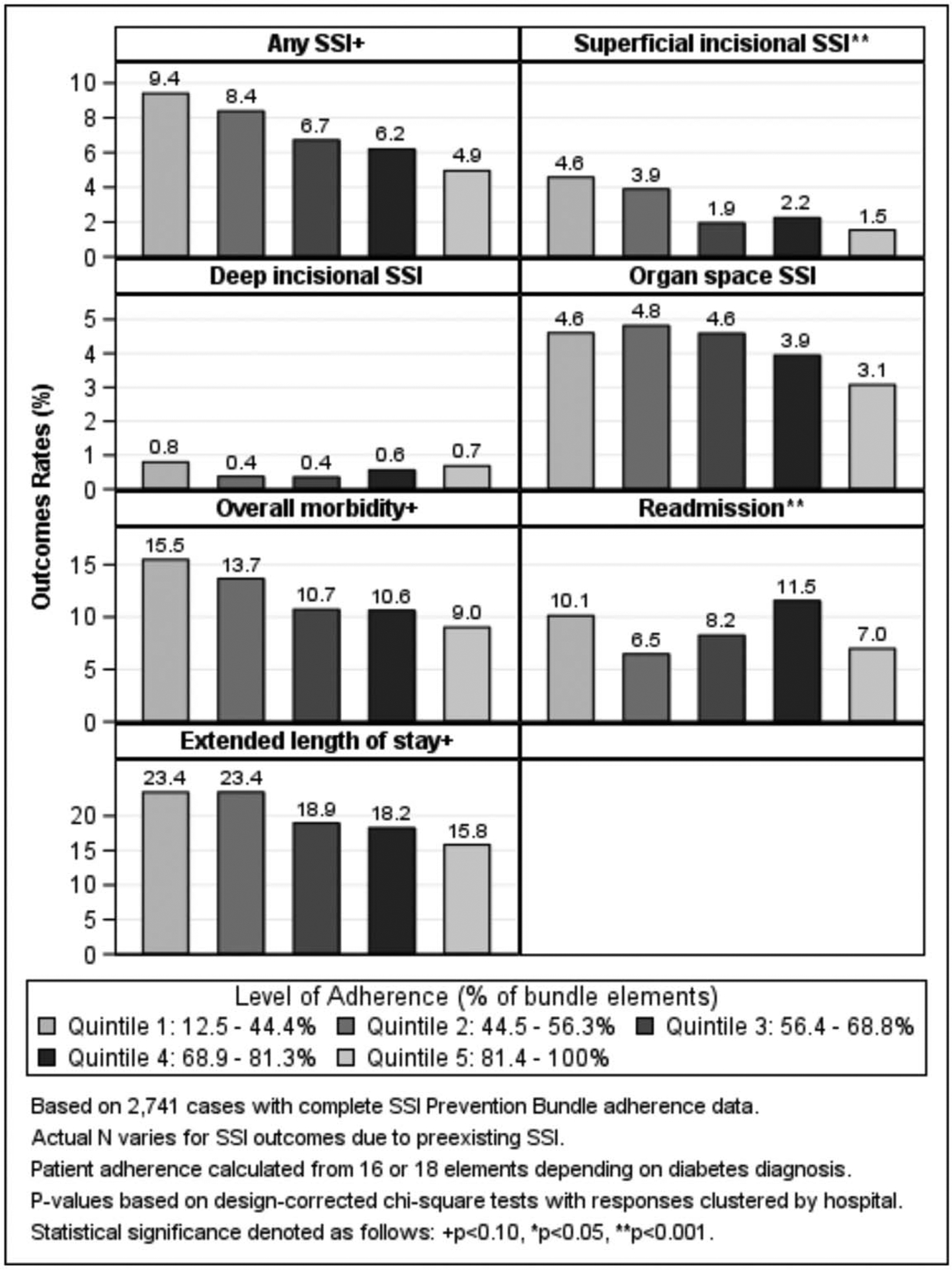
Results: Among 32 hospitals, there was a 2.5-fold relative increase in the proportion of patients completing at least 75% of bundle elements (preimplementation = 19.5% vs. postimplementation = 49.8%, P = 0.001). Largest adherence gains were seen in wound closure re-gowning/re-gloving (24.0% vs. 62.0%, P < 0.001), use of clean closing instruments (32.1% vs. 66.2%, P = 0.003), and preoperative chlorhexidine bathing (46.1% vs. 77.6%, P < 0.001). Multivariable analyses showed a trend toward lower risk of superficial incisional SSI in the postimplementation period compared to baseline (OR 0.70, 95% CI 0.49-10.2, P = 0.06). As the adherence in the number of bundle elements increased, there was a significant decrease in superficial SSI rates (lowest adherence quintile, 4.6% vs. highest, 1.5%, P < 0.001).
Conclusions: A comprehensive multifaceted SSI reduction bundle can be successfully implemented throughout a large quality improvement learning collaborative when coordinated quality improvement activities are leveraged, resulting in a 30% decline in SSI rates. Lower superficial SSI rates are associated with the number of adherent bundle elements a patient receives, rendering considerable benefits to institutions capable of implementing more components of the bundle.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Allegranzi B, Bagheri Nejad S, Combescure C, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011;377:228–241. - PubMed
-
- Badia JM, Casey AL, Petrosillo N, et al. Impact of surgical site infection on healthcare costs and patient outcomes: a systematic review in six European countries. J Hosp Infect. 2017;96:1–15. - PubMed
-
- Astagneau P, Rioux C, Golliot F, et al. Morbidity and mortality associated with surgical site infections: results from the 1997–1999 INCISO surveillance. J Hosp Infect. 2001;48:267–274. - PubMed
-
- Gantz O, Zagadailov P, Merchant AM. The cost of surgical site infections after colorectal surgery in the United States from 2001 to 2012: a longitudinal analysis. Am Surg. 2019;85:142–149. - PubMed
-
- Merkow RP, Ju MH, Chung JW, et al. Underlying reasons associated with hospital readmission following surgery in the United States. JAMA. 2015;313:483–495. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
