

Performance of Two-Stage Cervical Cancer Screening With Primary High-Risk Human Papillomavirus Testing in Women Living With Human Immunodeficiency Virus
- PMID: 31503167
- PMCID: PMC6768725
- DOI: 10.1097/AOG.0000000000003496
Performance of Two-Stage Cervical Cancer Screening With Primary High-Risk Human Papillomavirus Testing in Women Living With Human Immunodeficiency Virus
Abstract
Objective: To evaluate the performance of cervical cancer screening algorithms for women living with human immunodeficiency virus (HIV), using primary high-risk human papillomavirus (HPV) testing followed by cytology, visual inspection with acetic acid, or colposcopy.
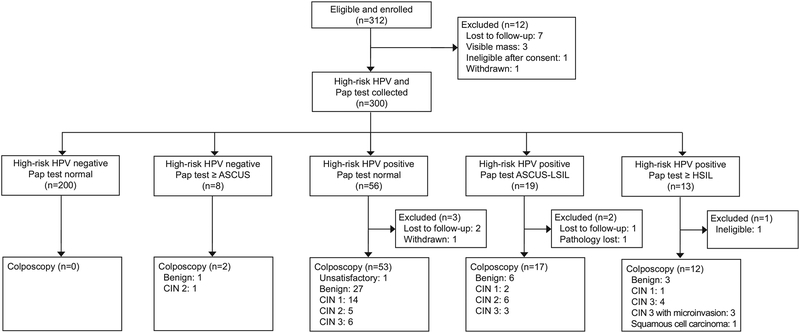
Methods: We conducted a prospective cohort study of women living with HIV in Botswana. All participants underwent high-risk HPV testing. Participants with positive high-risk HPV test results underwent cytology, visual inspection with acetic acid, colposcopy, and biopsy. Participants with negative high-risk HPV test results also underwent cytology. Histopathology was the reference standard for determination of preinvasive cervical disease and cervical cancer. Sensitivity, specificity, positive predictive value (PPV), negative predictive value, and likelihood ratios (LR) of high-risk HPV-based two-stage screening algorithms were calculated.
Results: Among 300 women screened, 88 (29%) had a positive high-risk HPV test result, and 29 of the 88 (35%) women who tested positive for high-risk HPV had CIN 2 or higher on histopathology. High-risk HPV followed by colposcopy resulted in a sensitivity of 83%, specificity of 49%, PPV of 47%, LR+ of +1.6, and LR- of -0.4. High-risk HPV followed by visual inspection with acetic acid resulted in a reduced sensitivity of 59%, specificity of 49%, PPV of 39%, LR+ of +1.2, and LR- of -0.8. High-risk HPV testing followed by cytology also resulted in a reduced sensitivity of 62%, specificity of 77%, PPV of 60%, LR+ of +2.7, and LR- of -0.5. Stratification by HPV 16/18/45 did not improve performance of the algorithms.
Conclusion: In a high-risk population with HIV, high-risk HPV testing followed by colposcopy demonstrated the highest sensitivity and PPV in detecting high-grade cervical dysplasia. Allocating resources to colposcopy in resource-limited settings may be more effective than other screening strategies.
Conflict of interest statement
Financial Disclosure
The authors did not report any potential conflicts of interest.
Figures
References
-
- World Health Organization. Botswana, Cancer Country Profile. WHO, 2014, http://who.int/cancer/country-profiles/bwa_en.pdf. Accessed 17 April 2019.
-
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F (2013). GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer; Available from http://globocan.iarc.fr.
-
- Torre L, Bray F, Siegel R, Ferlay J, Lortet-Tieulent J, Ahmedin J. Global cancer statistics, 2012. CA Cancer J Clin, 2015;65:87–108. - PubMed
-
- Ellerbrock T, Chiasson M, Bush T, Sun X, Sawo D, Brudney K. Incidence of cervical squamous intraepithelial lesions in HIV-infected women. JAMA, 2000; 283(8):1031. - PubMed
