

Effect of Corticosteroid-Sparing Treatment With Mycophenolate Mofetil vs Methotrexate on Inflammation in Patients With Uveitis: A Randomized Clinical Trial
- PMID: 31503307
- PMCID: PMC6737523
- DOI: 10.1001/jama.2019.12618
Effect of Corticosteroid-Sparing Treatment With Mycophenolate Mofetil vs Methotrexate on Inflammation in Patients With Uveitis: A Randomized Clinical Trial
Abstract
Importance: Methotrexate and mycophenolate mofetil are commonly used immunomodulatory therapies for achieving corticosteroid-sparing control of noninfectious uveitis, but there is uncertainty about which drug is more effective.
Objective: To compare the effect of methotrexate and mycophenolate for achieving corticosteroid-sparing control of noninfectious intermediate uveitis, posterior uveitis, and panuveitis.
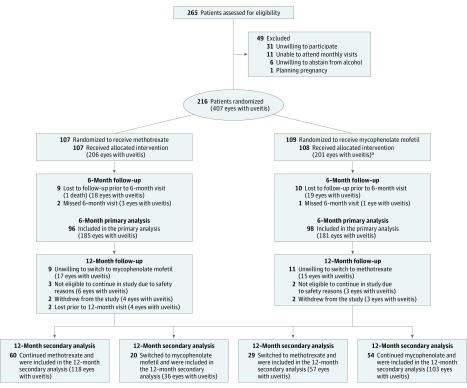
Design, setting, and participants: The First-line Antimetabolites as Steroid-sparing Treatment (FAST) uveitis trial screened 265 adults with noninfectious uveitis requiring corticosteroid-sparing immunosuppressive therapy from 9 referral eye centers in India, the United States, Australia, Saudi Arabia, and Mexico between August 22, 2013, and August 16, 2017. Follow-up ended on August 20, 2018.
Interventions: Patients were randomized to receive oral methotrexate, 25 mg weekly (n = 107), or oral mycophenolate mofetil, 3 g daily (n = 109).
Main outcomes and measures: The primary outcome was treatment success at 6 months, which was defined as having control of inflammation in both eyes, no more than 7.5 mg prednisone daily and less than or equal to 2 drops of prednisolone acetate 1%, and no treatment failure due to safety or intolerability. Patients underwent follow-up to 12 months while receiving the same treatment or switched to the other antimetabolite, depending on their 6-month outcome.
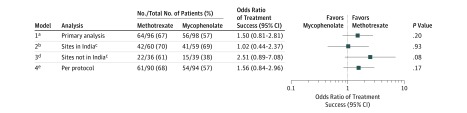
Results: Among 216 patients who were randomized (median age, 38 years; 135 (62.5%) women), 194 (89.8%) completed follow-up through 6 months. Treatment success occurred in 64 (66.7%) patients in the methotrexate group vs 56 (57.1%) in the mycophenolate group (difference, 9.5% [95% CI, -5.3% to 21.8%]; odds ratio [OR], 1.50 [95% CI, 0.81 to 2.81]; P = .20). Among patients with posterior uveitis or panuveitis, treatment success was achieved in 58 (74.4%) in the methotrexate group vs 42 (55.3%) in the mycophenolate group (difference, 19.1% [95% CI, 3.6% to 30.6%]; OR, 2.35 [95% CI, 1.16 to 4.90]; P = .02); whereas among patients with intermediate uveitis treatment success occurred in 6 (33.3%) in the methotrexate group vs 14 (63.6%) in the mycophenolate group (difference, -30.3% [95% CI, -51.6% to 1.1%]; OR, 0.29 [95% CI, 0.08 to 1.05]; P = .07; P for interaction = .004). Elevated liver enzymes were the most common nonserious laboratory adverse event, occurring in 14 patients (13.0%) in the methotrexate group and 8 patients (7.4%) in the mycophenolate group.
Conclusions and relevance: Among adults with noninfectious uveitis, the use of mycophenolate mofetil compared with methotrexate as first-line corticosteroid-sparing treatment did not result in superior control of inflammation. Further research is needed to determine if either drug is more effective based on the anatomical subtype of uveitis.
Trial registration: ClinicalTrials.gov Identifier: NCT01829295.
Conflict of interest statement
Figures
Comment in
-
Antimetabolite Therapy for Uveitis: Methotrexate or Mycophenolate?JAMA Ophthalmol. 2019 Dec 1;137(12):1449-1451. doi: 10.1001/jamaophthalmol.2019.3964. JAMA Ophthalmol. 2019. PMID: 31503274 No abstract available.
-
Stratification Clarification for Methods for Randomized Clinical Trials.JAMA Ophthalmol. 2020 Jul 1;138(7):800-801. doi: 10.1001/jamaophthalmol.2020.1551. JAMA Ophthalmol. 2020. PMID: 32437493 No abstract available.
-
Stratification Clarification for Methods for Randomized Clinical Trials-Reply.JAMA Ophthalmol. 2020 Jul 1;138(7):801. doi: 10.1001/jamaophthalmol.2020.1864. JAMA Ophthalmol. 2020. PMID: 32437500 Free PMC article. No abstract available.
