

Association Between Dialysis Facility Ownership and Access to Kidney Transplantation
- PMID: 31503308
- PMCID: PMC6737748
- DOI: 10.1001/jama.2019.12803
Association Between Dialysis Facility Ownership and Access to Kidney Transplantation
Retracted and republished in
-
Notice of Retraction and Replacement. Gander et al. Association Between Dialysis Facility Ownership and Access to Kidney Transplantation. JAMA. 2019;322(10):957-973.JAMA. 2020 Apr 21;323(15):1509-1510. doi: 10.1001/jama.2020.2328. JAMA. 2020. PMID: 32315061 Free PMC article.
Abstract
Importance: For-profit (vs nonprofit) dialysis facilities have historically had lower kidney transplantation rates, but it is unknown if the pattern holds for living donor and deceased donor kidney transplantation, varies by facility ownership, or has persisted over time in a nationally representative population.
Objective: To determine the association between dialysis facility ownership and placement on the deceased donor kidney transplantation waiting list, receipt of a living donor kidney transplant, or receipt of a deceased donor kidney transplant.
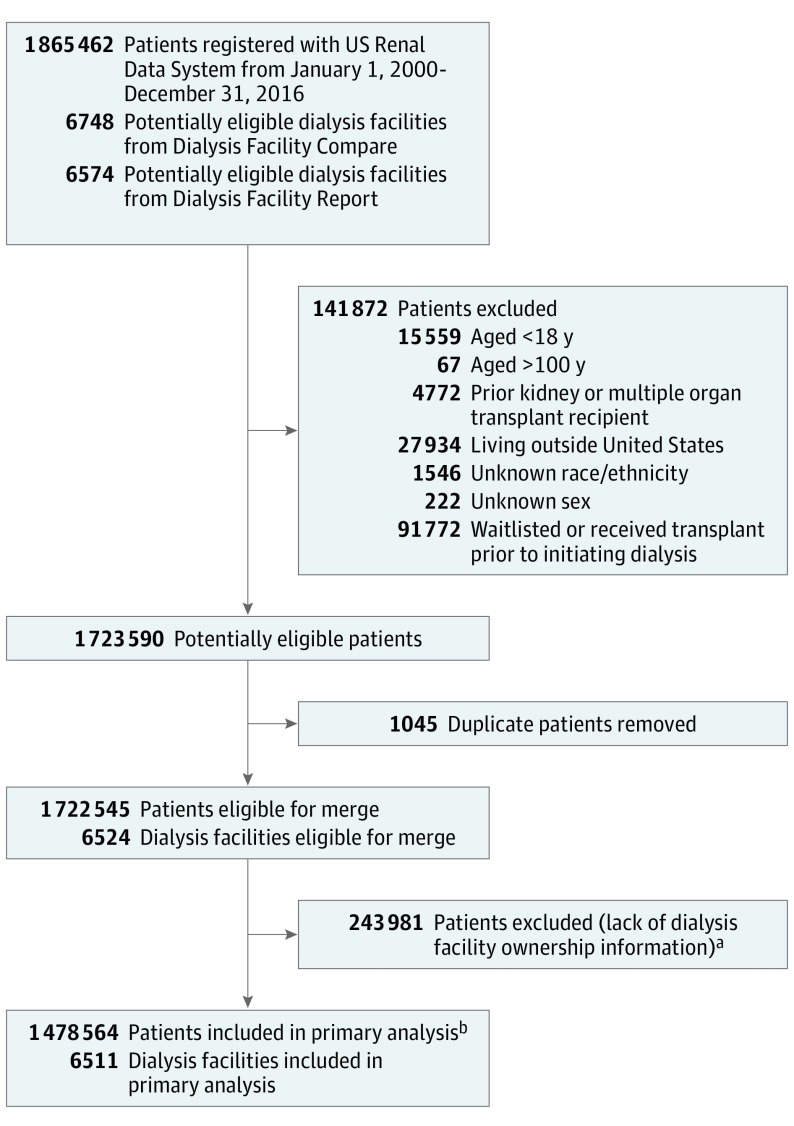
Design, setting, and participants: Retrospective cohort study that included 1 478 564 patients treated at 6511 US dialysis facilities. Adult patients with incident end-stage kidney disease from the US Renal Data System (2000-2016) were linked with facility ownership (Dialysis Facility Compare) and characteristics (Dialysis Facility Report).
Exposures: The primary exposure was dialysis facility ownership, which was categorized as nonprofit small chains, nonprofit independent facilities, for-profit large chains (>1000 facilities), for-profit small chains (<1000 facilities), and for-profit independent facilities.
Main outcomes and measures: Access to kidney transplantation was defined as time from initiation of dialysis to placement on the deceased donor kidney transplantation waiting list, receipt of a living donor kidney transplant, or receipt of a deceased donor kidney transplant. Cumulative incidence differences and multivariable Cox models assessed the association between dialysis facility ownership and each outcome.
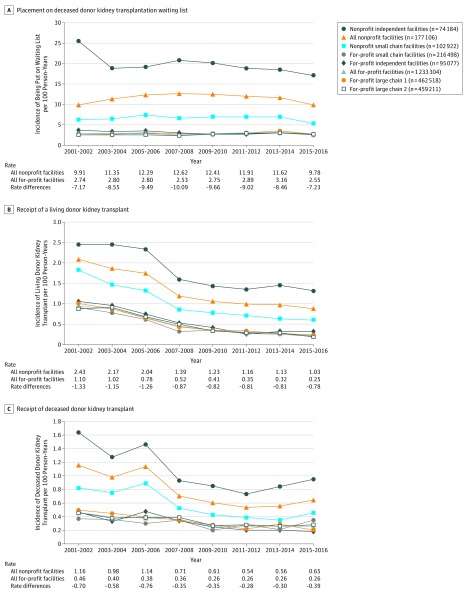
Results: Among 1 478 564 patients, the median age was 66 years (interquartile range, 55-76 years), with 55.3% male, and 28.1% non-Hispanic black patients. Eighty-seven percent of patients received care at a for-profit dialysis facility. A total of 109 030 patients (7.4%) received care at 435 nonprofit small chain facilities; 78 287 (5.3%) at 324 nonprofit independent facilities; 483 988 (32.7%) at 2239 facilities of large for-profit chain 1; 482 689 (32.6%) at 2082 facilities of large for-profit chain 2; 225 890 (15.3%) at 997 for-profit small chain facilities; and 98 680 (6.7%) at 434 for-profit independent facilities. During the study period, 121 680 patients (8.2%) were placed on the deceased donor waiting list, 23 762 (1.6%) received a living donor kidney transplant, and 49 290 (3.3%) received a deceased donor kidney transplant. For-profit facilities had lower 5-year cumulative incidence differences for each outcome vs nonprofit facilities (deceased donor waiting list: -13.2% [95% CI, -13.4% to -13.0%]; receipt of a living donor kidney transplant: -2.3% [95% CI, -2.4% to -2.3%]; and receipt of a deceased donor kidney transplant: -4.3% [95% CI, -4.4% to -4.2%]). Adjusted Cox analyses showed lower relative rates for each outcome among patients treated at all for-profit vs all nonprofit dialysis facilities: deceased donor waiting list (hazard ratio [HR], 0.36 [95% CI, 0.35 to 0.36]); receipt of a living donor kidney transplant (HR, 0.52 [95% CI, 0.51 to 0.54]); and receipt of a deceased donor kidney transplant (HR, 0.44 [95% CI, 0.44 to 0.45]).
Conclusions and relevance: Among US patients with end-stage kidney disease, receiving dialysis at for-profit facilities compared with nonprofit facilities was associated with a lower likelihood of accessing kidney transplantation. Further research is needed to understand the mechanisms behind this association.
Conflict of interest statement
Figures
Comment in
-
Improving Access to Kidney Transplantation: Business as Usual or New Ways of Doing Business?JAMA. 2019 Sep 10;322(10):931-933. doi: 10.1001/jama.2019.12784. JAMA. 2019. PMID: 31503296 No abstract available.
-
Re: Association between Dialysis Facility Ownership and Access to Kidney Transplantation.J Urol. 2020 Mar;203(3):455. doi: 10.1097/JU.0000000000000672.01. Epub 2019 Dec 3. J Urol. 2020. PMID: 31793825 No abstract available.
References
-
- US Renal Data System US Renal Data System 2018 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2018.
-
- Office of the Federal Register; National Archives and Records Administration Conditions for coverage for ESRD facilities; 2008. https://www.govinfo.gov/app/details/FR-2008-04-15/08-1102. Accessed August 8, 2019.
-
- Department of Health and Human Services; Centers for Medicare & Medicaid Services End-stage renal disease medical evidence report: Medicare entitlement and/or patient registration; 2005. https://secure.ssa.gov/apps10/poms/images/Other/G-CMS-2728-U3-1.pdf. Accessed August 8, 2019.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
