

Myelopreservation with the CDK4/6 inhibitor trilaciclib in patients with small-cell lung cancer receiving first-line chemotherapy: a phase Ib/randomized phase II trial
- PMID: 31504118
- PMCID: PMC6857609
- DOI: 10.1093/annonc/mdz278
Myelopreservation with the CDK4/6 inhibitor trilaciclib in patients with small-cell lung cancer receiving first-line chemotherapy: a phase Ib/randomized phase II trial
Abstract
Background: Chemotherapy-induced damage of hematopoietic stem and progenitor cells (HSPC) causes multi-lineage myelosuppression. Trilaciclib is an intravenous CDK4/6 inhibitor in development to proactively preserve HSPC and immune system function during chemotherapy (myelopreservation). Preclinically, trilaciclib transiently maintains HSPC in G1 arrest and protects them from chemotherapy damage, leading to faster hematopoietic recovery and enhanced antitumor immunity.
Patients and methods: This was a phase Ib (open-label, dose-finding) and phase II (randomized, double-blind placebo-controlled) study of the safety, efficacy and PK of trilaciclib in combination with etoposide/carboplatin (E/P) therapy for treatment-naive extensive-stage small-cell lung cancer patients. Patients received trilaciclib or placebo before E/P on days 1-3 of each cycle. Select end points were prespecified to assess the effect of trilaciclib on myelosuppression and antitumor efficacy.
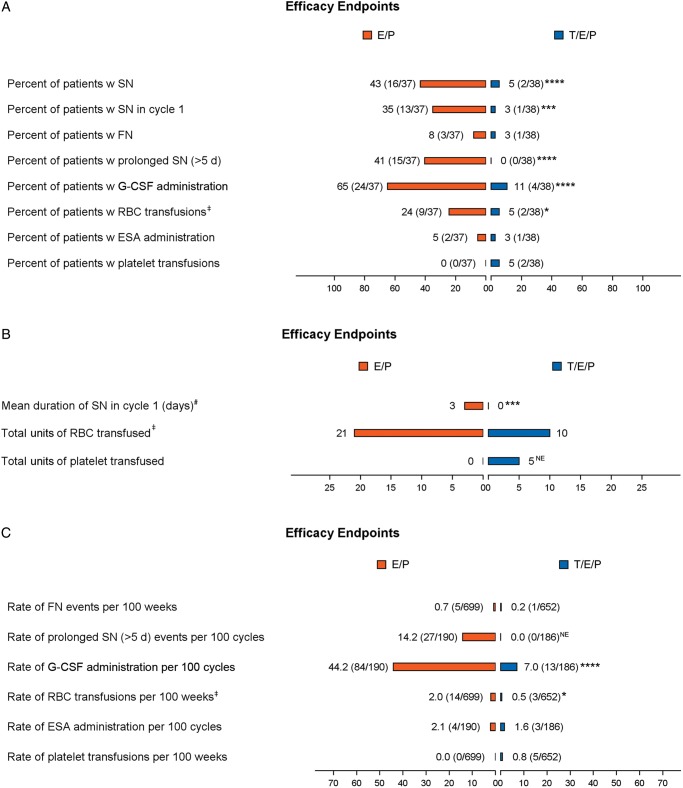
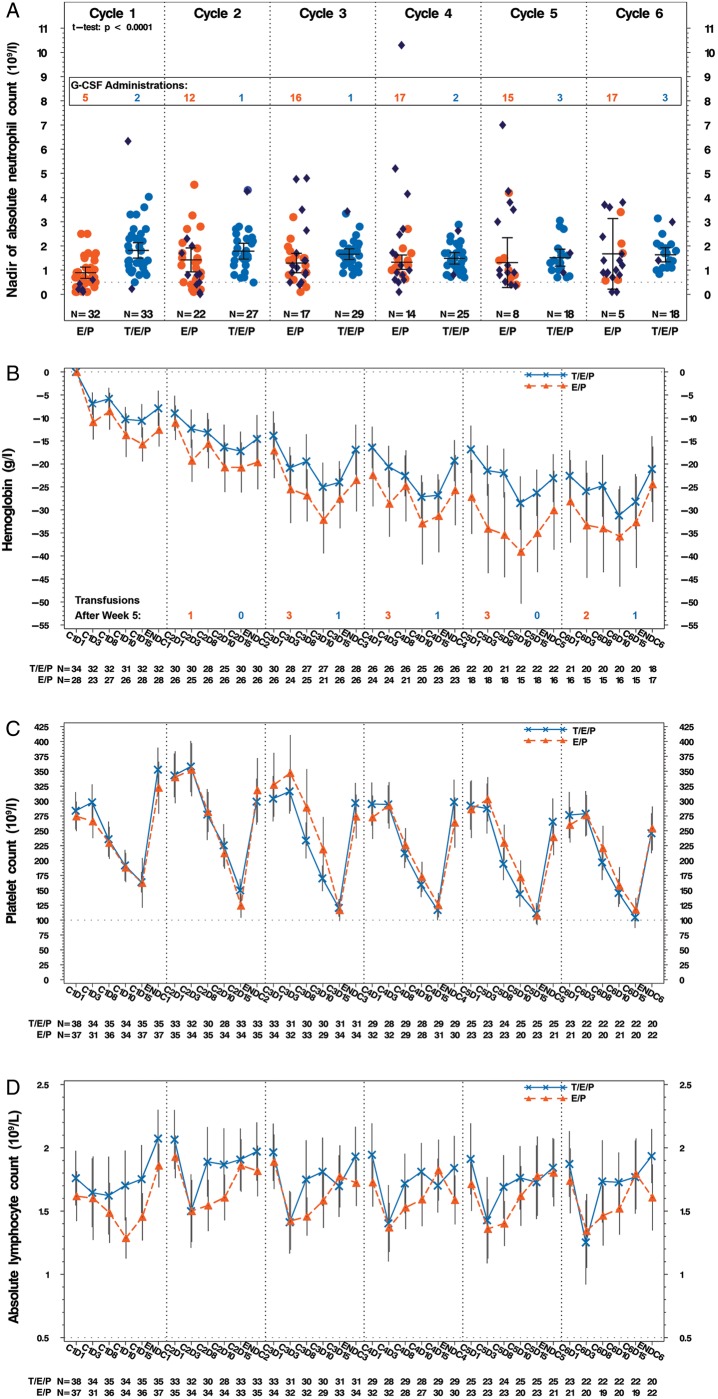
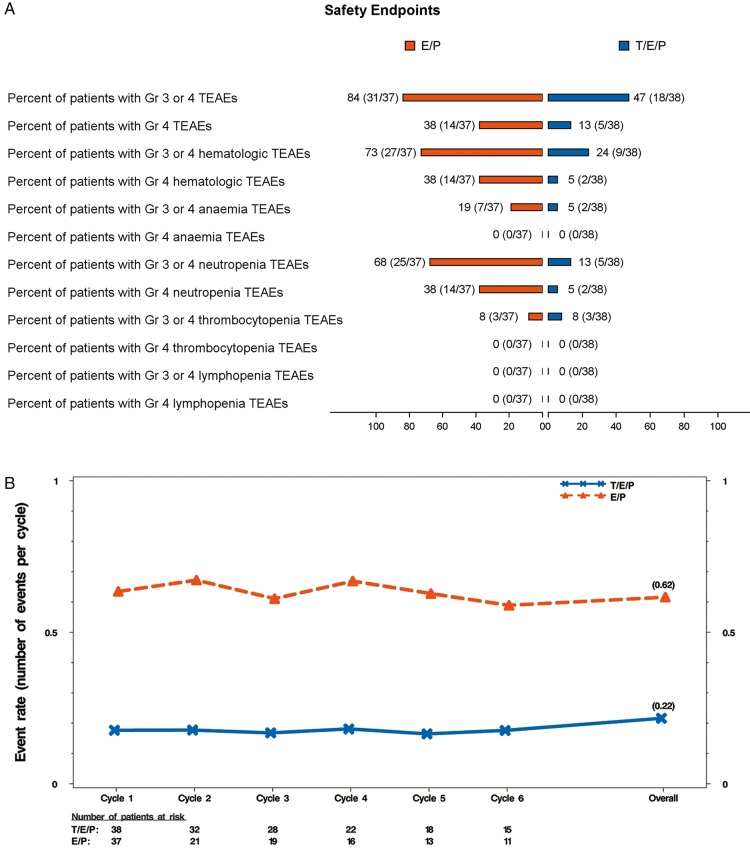
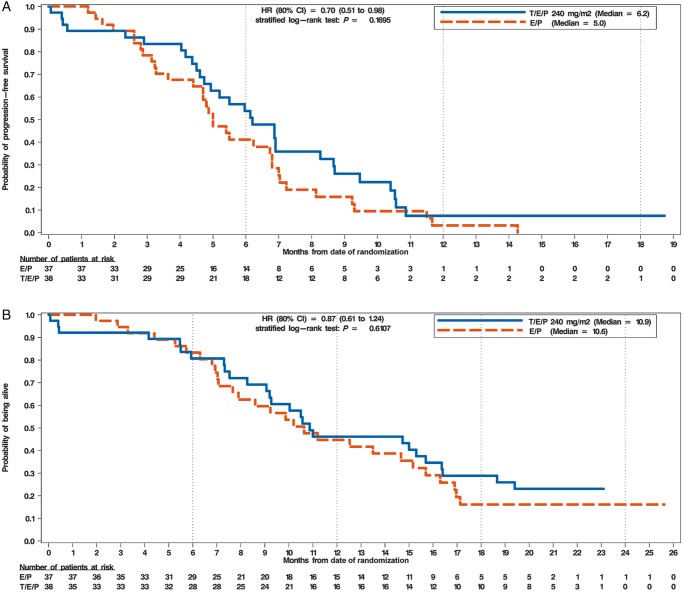
Results: A total of 122 patients were enrolled, with 19 patients in part 1 and 75 patients in part 2 receiving study drug. Improvements were seen with trilaciclib in neutrophil, RBC (red blood cell) and lymphocyte measures. Safety on trilaciclib+E/P was improved with fewer ≥G3 adverse events (AEs) in trilaciclib (50%) versus placebo (83.8%), primarily due to less hematological toxicity. No trilaciclib-related ≥G3 AEs occurred. Antitumor efficacy assessment for trilaciclib versus placebo, respectively, showed: ORR (66.7% versus 56.8%, P = 0.3831); median PFS [6.2 versus 5.0 m; hazard ratio (HR) 0.71; P = 0.1695]; and OS (10.9 versus 10.6 m; HR 0.87; P = 0.6107).
Conclusion: Trilaciclib demonstrated an improvement in the patient's tolerability of chemotherapy as shown by myelopreservation across multiple hematopoietic lineages resulting in fewer supportive care interventions and dose reductions, improved safety profile, and no detriment to antitumor efficacy. These data demonstrate strong proof-of-concept for trilaciclib's myelopreservation benefits.
Clinical trail number: NCT02499770.
Keywords: CDK4/6; anemia; myelopreservation; neutropenia; small-cell lung cancer; trilaciclib.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society for Medical Oncology.
Figures
References
-
- Bisi JE, Sorrentino JA, Roberts PJ. et al. Preclinical characterization of G1T28: a novel CDK4/6 inhibitor for reduction of chemotherapy-induced myelosuppression. Mol Cancer Ther 2016; 15(5): 783–793. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
