

Sputum Gram Stain for Bacterial Pathogen Diagnosis in Community-acquired Pneumonia: A Systematic Review and Bayesian Meta-analysis of Diagnostic Accuracy and Yield
- PMID: 31504334
- PMCID: PMC7384319
- DOI: 10.1093/cid/ciz876
Sputum Gram Stain for Bacterial Pathogen Diagnosis in Community-acquired Pneumonia: A Systematic Review and Bayesian Meta-analysis of Diagnostic Accuracy and Yield
Abstract
Background: The clinical role of sputum Gram stain (SGS) in community-acquired pneumonia (CAP) diagnosis remains controversial. A 1996 meta-analysis of the diagnostic accuracy of SGS reported heterogeneous results. To update the available evidence, we performed a systematic review and a Bayesian standard and latent-class model meta-analysis.
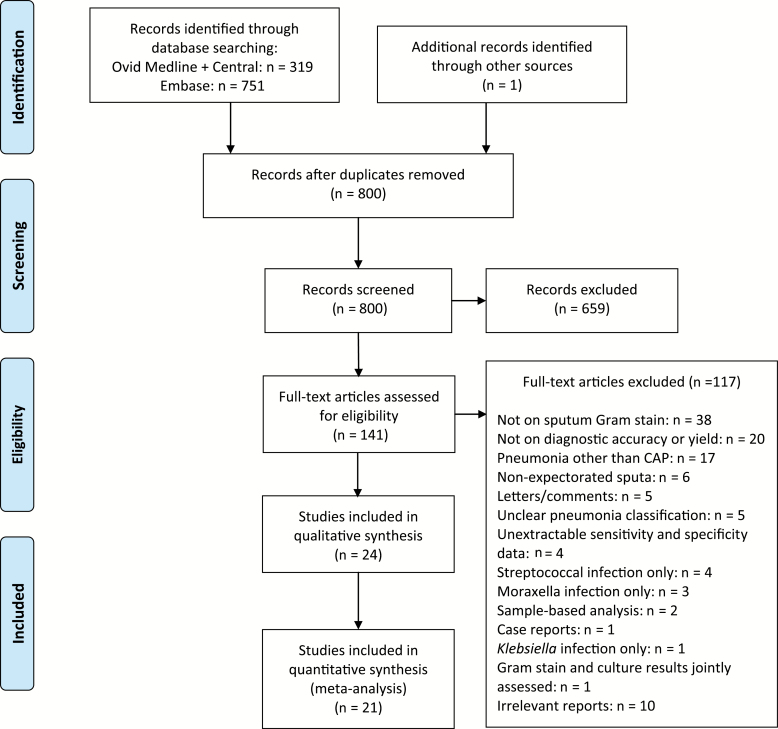
Methods: We searched Medline, Embase, and Cochrane Central by 23 August 2018 to identify studies reporting on the diagnostic accuracy, yield (percentage of patients with any pathogen[s] correctly identified by SGS), and clinical outcomes of SGS in adult patients with CAP. Two reviewers extracted the data. We quantitatively synthesized the diagnostic accuracy and yield, and descriptively analyzed other outcomes.
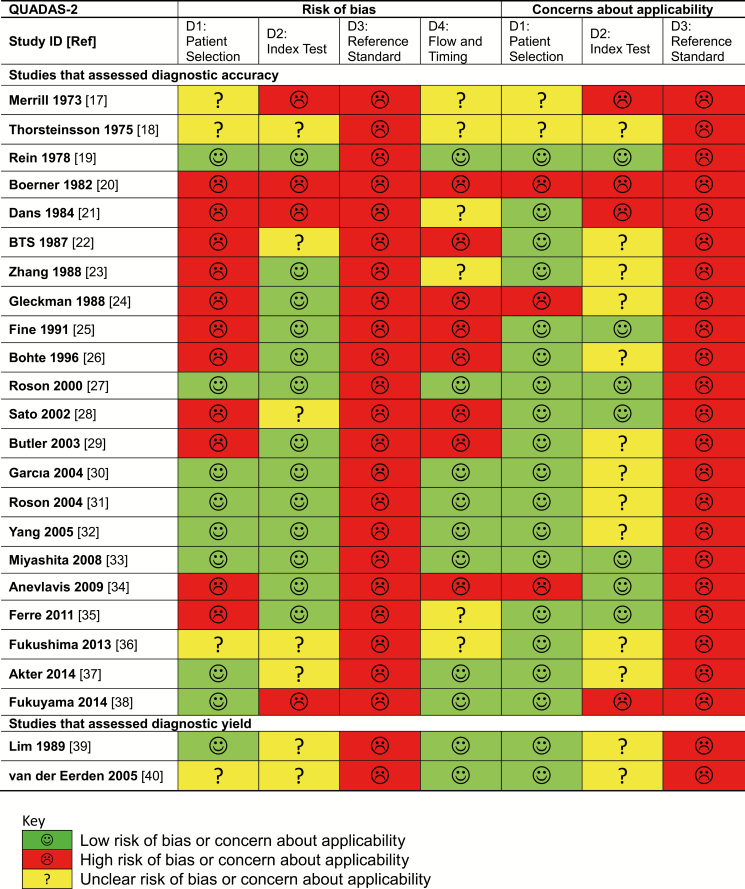
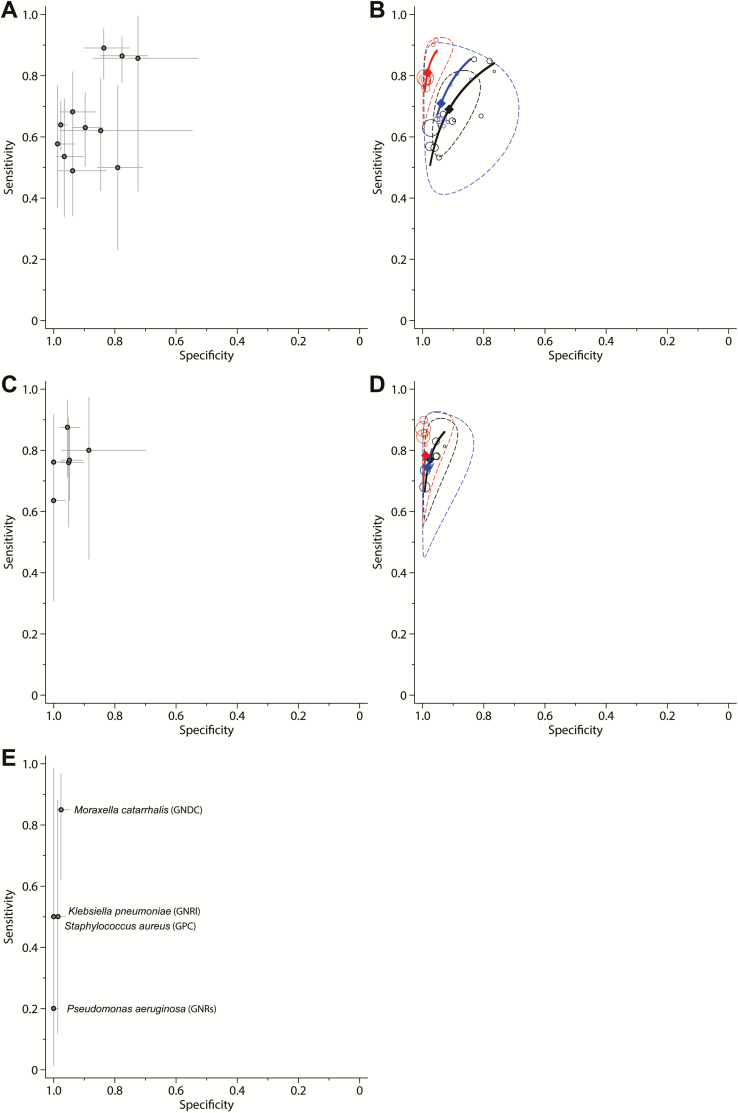
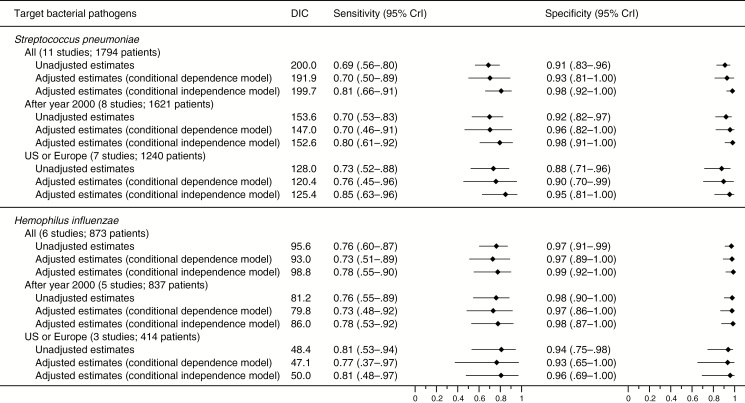
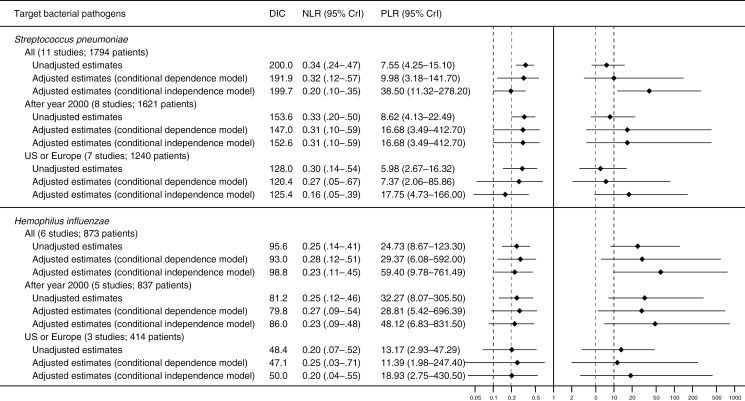
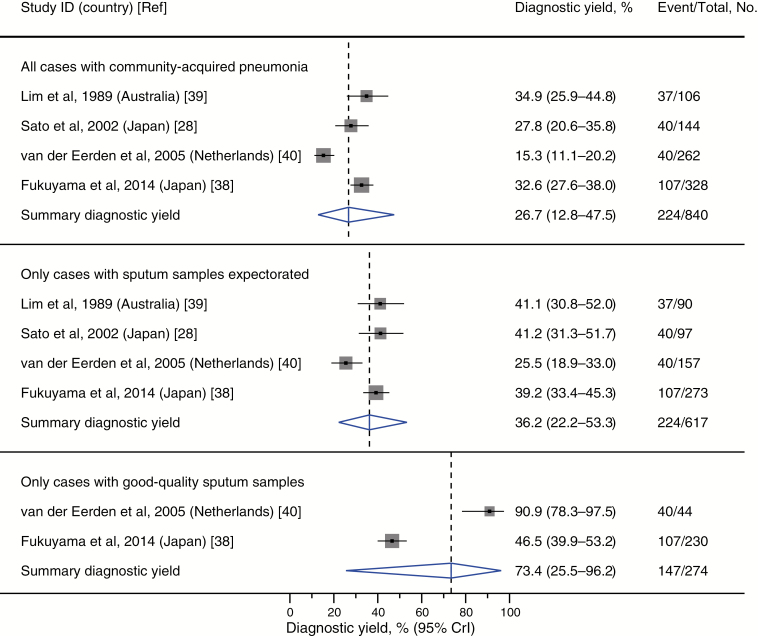
Results: Twenty-four studies with 4533 patients were included. The methodological and reporting quality of the included studies was limited. When good-quality sputum specimens were selected, SGS had a summary sensitivity of 0.69 (95% credible interval [CrI], .56-.80) and specificity of 0.91 (CrI, .83-.96) for detecting Streptococcus pneumoniae, and a sensitivity of 0.76 (CrI, .60-.87) and specificity of 0.97 (CrI, .91-.99) for Haemophilus influenzae. Adjusted analyses accounting for imperfect reference standards provided higher-specificity estimates than the unadjusted analyses. Bacterial pathogens were identified in 73% (CrI, 26%-96%) of good-quality specimens, and 36% (CrI, 22%-53%) of all specimens regardless of quality. Evidence on other bacteria was sparse.
Conclusions: SGS was highly specific to diagnose S. pneumoniae and H. influenzae infections in patients with CAP. With good-quality specimens, SGS can provide clinically actionable information for pathogen-directed antibiotic therapies.
Keywords: community-acquired pneumonia; diagnosis; meta-analysis; sensitivity and specificity; sputum Gram stain.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Challenges and Progress Toward Determining Pneumonia Etiology.Clin Infect Dis. 2020 Jul 27;71(3):514-516. doi: 10.1093/cid/ciz879. Clin Infect Dis. 2020. PMID: 31504351 No abstract available.
-
Microscopic Screening of Sputum Samples Should not be Used when Testing for Legionella Species.Clin Infect Dis. 2020 Aug 22;71(5):1356-1357. doi: 10.1093/cid/ciz1148. Clin Infect Dis. 2020. PMID: 31760427 No abstract available.
-
Reply to Ito.Clin Infect Dis. 2021 Jul 1;73(1):e273-e274. doi: 10.1093/cid/ciaa1643. Clin Infect Dis. 2021. PMID: 33112957 No abstract available.
-
The Still-Unknown Worth of a Gram Stain for Pneumonia.Clin Infect Dis. 2021 Jul 1;73(1):e273. doi: 10.1093/cid/ciaa1642. Clin Infect Dis. 2021. PMID: 33112961 No abstract available.
-
Reply to Musher.Clin Infect Dis. 2021 Oct 5;73(7):e1768-e1769. doi: 10.1093/cid/ciaa1914. Clin Infect Dis. 2021. PMID: 33388747 No abstract available.
-
Microscopic Examination of Gram-Stained Sputum: A Neglected Laboratory Modality.Clin Infect Dis. 2021 Oct 5;73(7):e1767-e1768. doi: 10.1093/cid/ciaa1913. Clin Infect Dis. 2021. PMID: 34363085 No abstract available.
References
-
- Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007; 44(Suppl 2):S27–72. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
