

Prospective International Study of Incidence and Predictors of Immune Reconstitution Inflammatory Syndrome and Death in People Living With Human Immunodeficiency Virus and Severe Lymphopenia
- PMID: 31504347
- PMCID: PMC7384325
- DOI: 10.1093/cid/ciz877
Prospective International Study of Incidence and Predictors of Immune Reconstitution Inflammatory Syndrome and Death in People Living With Human Immunodeficiency Virus and Severe Lymphopenia
Abstract
Background: Patients living with human immunodeficiency virus (PLWH) with low CD4 counts are at high risk for immune reconstitution inflammatory syndrome (IRIS) and death at antiretroviral therapy (ART) initiation.
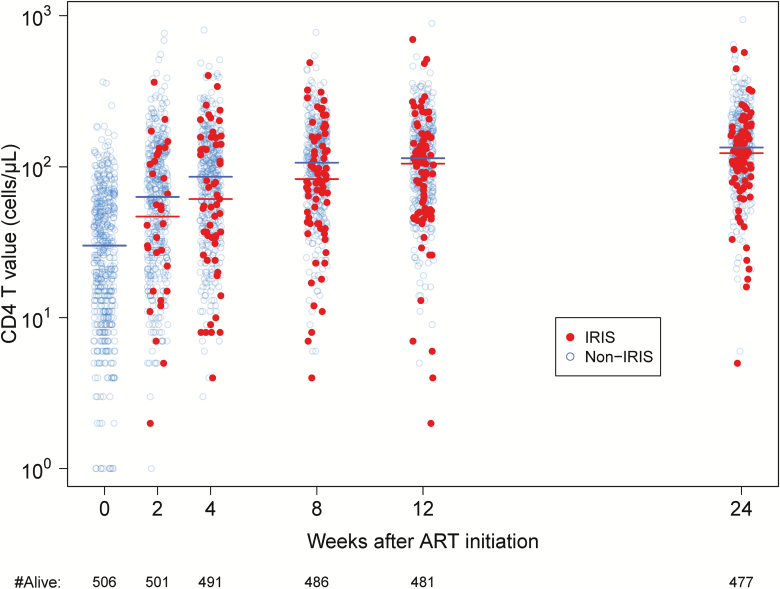
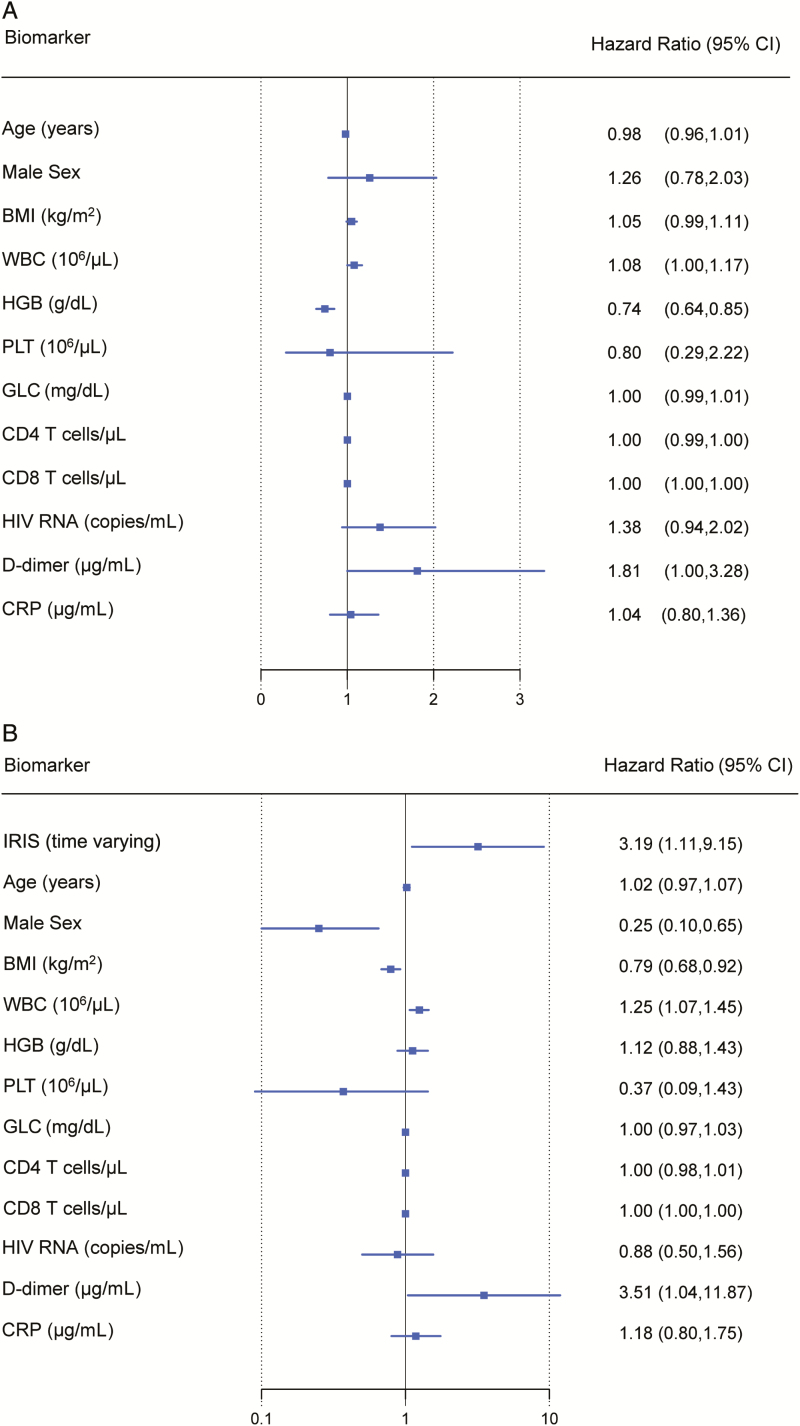
Methods: We investigated the clinical impact of IRIS in PLWH and CD4 counts <100 cells/μL starting ART in an international, prospective study in the United States, Thailand, and Kenya. An independent review committee adjudicated IRIS events. We assessed associations between baseline biomarkers, IRIS, immune recovery at week 48, and death by week 48 with Cox models.
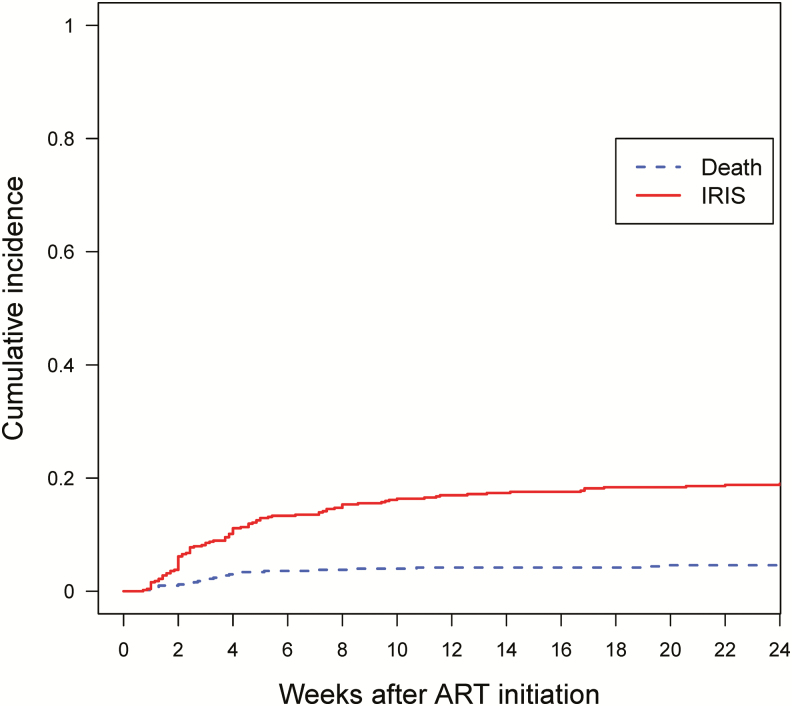
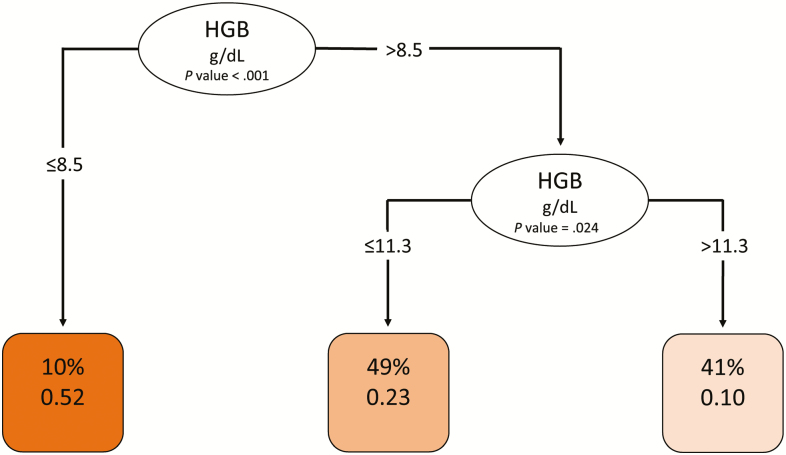
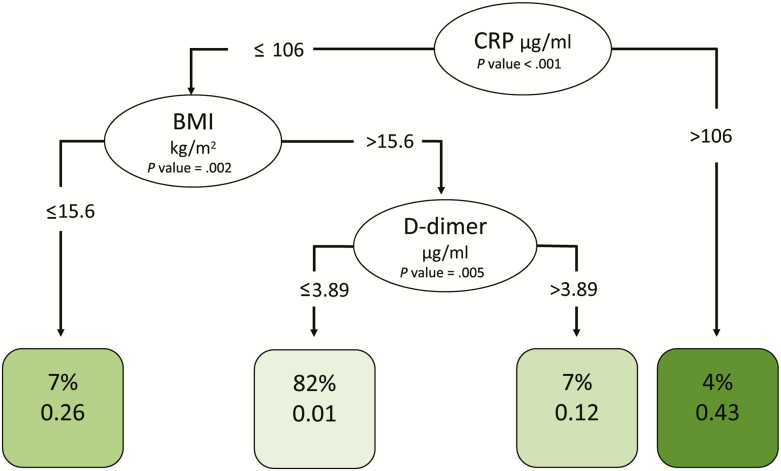
Results: We enrolled 506 participants (39.3% were women). Median age was 37 years, and CD4 count was 29 cells/μL. Within 6 months of ART, 97 (19.2%) participants developed IRIS and 31 (6.5%) died. Participants with lower hemoglobin at baseline were at higher IRIS risk (hazard ratio [HR], 1.2; P = .004). IRIS was independently associated with increased risk of death after adjustment for known risk factors (HR, 3.2; P = .031). Being female (P = .004) and having a lower body mass index (BMI; P = .003), higher white blood cell count (P = .005), and higher D-dimer levels (P = .044) were also significantly associated with increased risk of death. Decision-tree analysis identified hemoglobin <8.5 g/dL as predictive of IRIS and C-reactive protein (CRP) >106 μg/mL and BMI <15.6 kg/m2 as predictive of death.
Conclusions: For PLWH with severe immunosuppression initiating ART, baseline low BMI and hemoglobin and high CRP and D-dimer levels may be clinically useful predictors of IRIS and death risk.
Keywords: AIDS; HIV; biomarkers; death; immune reconstitution inflammatory syndrome (IRIS).
Published by Oxford University Press for the Infectious Diseases Society of America 2019.
Figures
References
-
- Danel C, Moh R, Gabillard D, et al. ; TEMPRANO ANRS 12136 Study Group A trial of early antiretrovirals and isoniazid preventive therapy in Africa. N Engl J Med 2015; 373:808–22. - PubMed
-
- Recommendations regarding provision of ART for all persons living with HIV (Test and START): PEPFAR Scientific Advisory Board. 2015. Available at: https://www.pepfar.gov/documents/organization/250048.pdf.
-
- Prevent HIV, Test and Treat All. Progress Report 2016. WHO Support for Country Impact. Geneva, Switzerland: World Health Organization, 2016.
-
- PoAGfAaA GftUoAAiA, Available at: https://aidsinfo.nih.gov/guidelines/html/1/adult-and-adolescentarv/10/in.... Accessed 13 September 2019.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
