

Mortality reduction with physical activity in patients with and without cardiovascular disease
- PMID: 31504416
- PMCID: PMC6855138
- DOI: 10.1093/eurheartj/ehz564
Mortality reduction with physical activity in patients with and without cardiovascular disease
Abstract
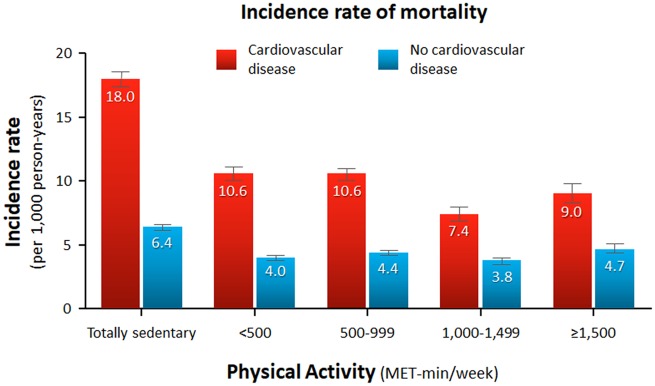
Aims: Physical activity has been shown to reduce mortality in a dose-response fashion. Current guidelines recommend 500-1000 metabolic equivalent task (MET)-min per week of regular physical activity. This study aimed to compare the impact of leisure-time physical activity on mortality in primary versus secondary cardiovascular prevention.
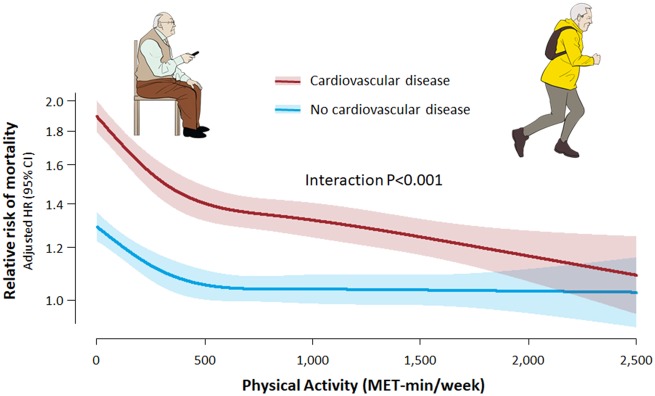
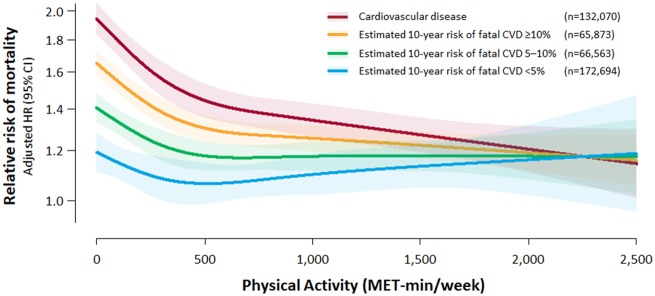
Methods and results: This study included a total of 131 558 and 310 240 subjects with and without cardiovascular disease (CVD), respectively, from a population-based cohort. Leisure-time physical activity was measured by self-report questionnaires. The study subjects were followed-up for a median of 5.9 years, and the main study outcome was all-cause mortality. There was an inverse relationship between the physical activity level and the mortality risk in both groups. The benefit in the secondary prevention group was shown to be greater than that in the primary prevention group: every 500 MET-min/week increase in physical activity resulted in a 14% and 7% risk reduction in mortality in the secondary and primary prevention groups, respectively (interaction P < 0.001). In addition, while individuals without CVD benefited the most between 1 and 500 MET-min/week of physical activity, the benefit in those with CVD continued above 500 - 1000 MET-min/week. The adjusted mortality risk of individuals with CVD who performed a high level of physical activity (≥1000 MET-min/week) was shown to be comparable to or lower than that of their counterparts without CVD.
Conclusion: Individuals with CVD may benefit from physical activity to a greater extent than do healthy subjects without CVD.
Keywords: Cohort study; Exercise; Metabolic equivalent; Physical activity; Risk reduction behaviour; Secondary prevention.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

Comment in
-
Promoting physical activity in primary and secondary prevention.Eur Heart J. 2019 Nov 14;40(43):3556-3558. doi: 10.1093/eurheartj/ehz697. Eur Heart J. 2019. PMID: 31560038 No abstract available.
Similar articles
-
Beneficial associations of low and large doses of leisure time physical activity with all-cause, cardiovascular disease and cancer mortality: a national cohort study of 88,140 US adults.Br J Sports Med. 2019 Nov;53(22):1405-1411. doi: 10.1136/bjsports-2018-099254. Epub 2019 Mar 19. Br J Sports Med. 2019. PMID: 30890520
-
Physical activity in the prevention of cardiovascular disease: an epidemiological perspective.Sports Med. 2001 Feb;31(2):101-14. doi: 10.2165/00007256-200131020-00003. Sports Med. 2001. PMID: 11227978 Review.
-
Leisure Sedentary Behavior, Physical Activities, and Cardiovascular Disease Among Individuals With Metabolic Dysfunction-Associated Fatty Liver Disease.Arterioscler Thromb Vasc Biol. 2024 Sep;44(9):e227-e237. doi: 10.1161/ATVBAHA.124.321214. Epub 2024 Aug 1. Arterioscler Thromb Vasc Biol. 2024. PMID: 39087351
-
Long-Term Leisure-Time Physical Activity Intensity and All-Cause and Cause-Specific Mortality: A Prospective Cohort of US Adults.Circulation. 2022 Aug 16;146(7):523-534. doi: 10.1161/CIRCULATIONAHA.121.058162. Epub 2022 Jul 25. Circulation. 2022. PMID: 35876019 Free PMC article.
-
Associations of leisure-time physical activity with cardiovascular mortality: A systematic review and meta-analysis of 44 prospective cohort studies.Eur J Prev Cardiol. 2018 Nov;25(17):1864-1872. doi: 10.1177/2047487318795194. Epub 2018 Aug 30. Eur J Prev Cardiol. 2018. PMID: 30157685
Cited by
-
Using Bayesian networks with Max-Min Hill-Climbing algorithm to detect factors related to multimorbidity.Front Cardiovasc Med. 2022 Aug 30;9:984883. doi: 10.3389/fcvm.2022.984883. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36110415 Free PMC article.
-
Life's essential 8 and risk of all-cause mortality in individuals with cardiovascular diseases: A prospective community-based study.Clin Cardiol. 2024 Feb;47(2):e24119. doi: 10.1002/clc.24119. Epub 2023 Nov 23. Clin Cardiol. 2024. PMID: 37994466 Free PMC article.
-
Atrial Fibrillation Specific Exercise Rehabilitation: Are We There Yet?J Pers Med. 2022 Apr 10;12(4):610. doi: 10.3390/jpm12040610. J Pers Med. 2022. PMID: 35455726 Free PMC article. Review.
-
Designing a Randomized Trial with an Age Simulation Suit-Representing People with Health Impairments.Healthcare (Basel). 2020 Dec 30;9(1):27. doi: 10.3390/healthcare9010027. Healthcare (Basel). 2020. PMID: 33396686 Free PMC article.
-
Effectiveness of Mobile Health-Based Gamification Interventions for Improving Physical Activity in Individuals With Cardiovascular Diseases: Systematic Review and Meta-Analysis of Randomized Controlled Trials.JMIR Serious Games. 2025 Jan 24;13:e64410. doi: 10.2196/64410. JMIR Serious Games. 2025. PMID: 39854099 Free PMC article. Review.
References
-
- Moore SC, Patel AV, Matthews CE, Berrington de Gonzalez A, Park Y, Katki HA, Linet MS, Weiderpass E, Visvanathan K, Helzlsouer KJ, Thun M, Gapstur SM, Hartge P, Lee IM.. Leisure time physical activity of moderate to vigorous intensity and mortality: a large pooled cohort analysis. PLoS Med 2012;9:e1001335.. - PMC - PubMed
-
- Arem H, Moore SC, Patel A, Hartge P, Berrington de Gonzalez A, Visvanathan K, Campbell PT, Freedman M, Weiderpass E, Adami HO, Linet MS, Lee IM, Matthews CE.. Leisure time physical activity and mortality: a detailed pooled analysis of the dose-response relationship. JAMA Intern Med 2015;175:959–967. - PMC - PubMed
-
- Liu Y, Shu XO, Wen W, Saito E, Rahman MS, Tsugane S, Tamakoshi A, Xiang YB, Yuan JM, Gao YT, Tsuji I, Kanemura S, Nagata C, Shin MH, Pan WH, Koh WP, Sawada N, Cai H, Li HL, Tomata Y, Sugawara Y, Wada K, Ahn YO, Yoo KY, Ashan H, Chia KS, Boffetta P, Inoue M, Kang D, Potter JD, Zheng W.. Association of leisure-time physical activity with total and cause-specific mortality: a pooled analysis of nearly a half million adults in the Asia Cohort Consortium. Int J Epidemiol 2018;47:771–779. - PMC - PubMed
-
- Eckel RH, Jakicic JM, Ard JD, de Jesus JM, Houston Miller N, Hubbard VS, Lee IM, Lichtenstein AH, Loria CM, Millen BE, Nonas CA, Sacks FM, Smith SC Jr, Svetkey LP, Wadden TA, Yanovski SZ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2960–2984. - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, Cooney MT, Corra U, Cosyns B, Deaton C, Graham I, Hall MS, Hobbs FDR, Lochen ML, Lollgen H, Marques-Vidal P, Perk J, Prescott E, Redon J, Richter DJ, Sattar N, Smulders Y, Tiberi M, van der Worp HB, van Dis I, Verschuren WMM, Binno S; ESC Scientific Document Group. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts). Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016;37:2315–2381. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
