

EANO guideline on the diagnosis and treatment of vestibular schwannoma
- PMID: 31504802
- PMCID: PMC6954440
- DOI: 10.1093/neuonc/noz153
EANO guideline on the diagnosis and treatment of vestibular schwannoma
Abstract
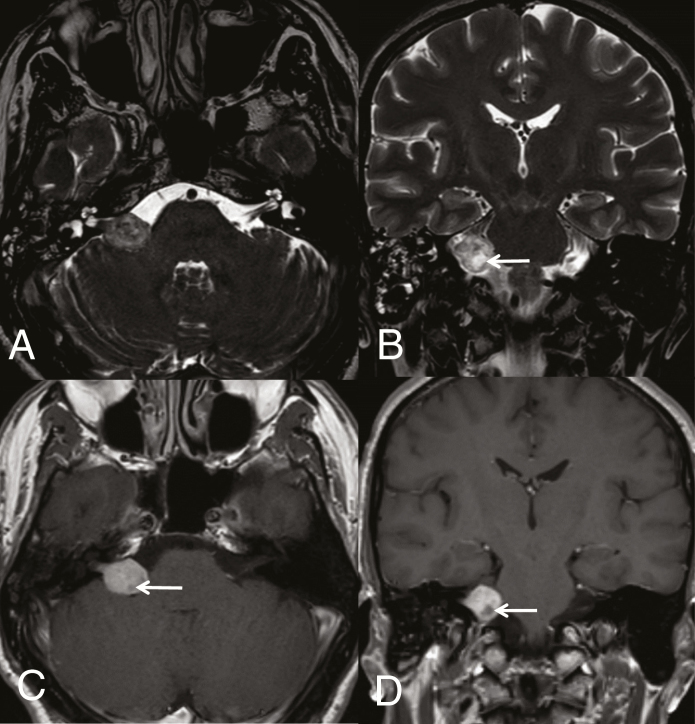
The level of evidence to provide treatment recommendations for vestibular schwannoma is low compared with other intracranial neoplasms. Therefore, the vestibular schwannoma task force of the European Association of Neuro-Oncology assessed the data available in the literature and composed a set of recommendations for health care professionals. The radiological diagnosis of vestibular schwannoma is made by magnetic resonance imaging. Histological verification of the diagnosis is not always required. Current treatment options include observation, surgical resection, fractionated radiotherapy, and radiosurgery. The choice of treatment depends on clinical presentation, tumor size, and expertise of the treating center. In small tumors, observation has to be weighed against radiosurgery, in large tumors surgical decompression is mandatory, potentially followed by fractionated radiotherapy or radiosurgery. Except for bevacizumab in neurofibromatosis type 2, there is no role for pharmacotherapy.
Keywords: diagnosis; radiotherapy; surgery; treatment; vestibular schwannoma.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Babu R, Sharma R, Bagley JH, Hatef J, Friedman AH, Adamson C. Vestibular schwannomas in the modern era: epidemiology, treatment trends, and disparities in management. J Neurosurg. 2013;119(1):121–130. - PubMed
-
- Jeyakumar A, Seth R, Brickman TM, Dutcher P. The prevalence and clinical course of patients with ‘incidental’ acoustic neuromas. Acta Otolaryngol. 2007;127(10):1051–1057. - PubMed
-
- Andersen JF, Nilsen KS, Vassbotn FS, et al. Predictors of vertigo in patients with untreated vestibular schwannoma. Otol Neurotol. 2015;36(4):647–652. - PubMed
-
- Kshettry VR, Hsieh JK, Ostrom QT, Kruchko C, Barnholtz-Sloan JS. Incidence of vestibular schwannomas in the United States. J Neurooncol. 2015;124(2):223–228. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
