

Pediatric Bacterial Meningitis Surveillance in Niger: Increased Importance of Neisseria meningitidis Serogroup C, and a Decrease in Streptococcus pneumoniae Following 13-Valent Pneumococcal Conjugate Vaccine Introduction
- PMID: 31505636
- PMCID: PMC6761310
- DOI: 10.1093/cid/ciz598
Pediatric Bacterial Meningitis Surveillance in Niger: Increased Importance of Neisseria meningitidis Serogroup C, and a Decrease in Streptococcus pneumoniae Following 13-Valent Pneumococcal Conjugate Vaccine Introduction
Abstract
Background: Meningitis is endemic in Niger. Haemophilus influenzae type b (Hib) vaccine and the 13-valent pneumococcal conjugate vaccine (PCV13) were introduced in 2008 and 2014, respectively. Vaccination campaign against Neisseria meningitidis serogroup A was carried out in 2010-2011. We evaluated changes in pathogen distribution using data from hospital-based surveillance in Niger from 2010 through 2016.
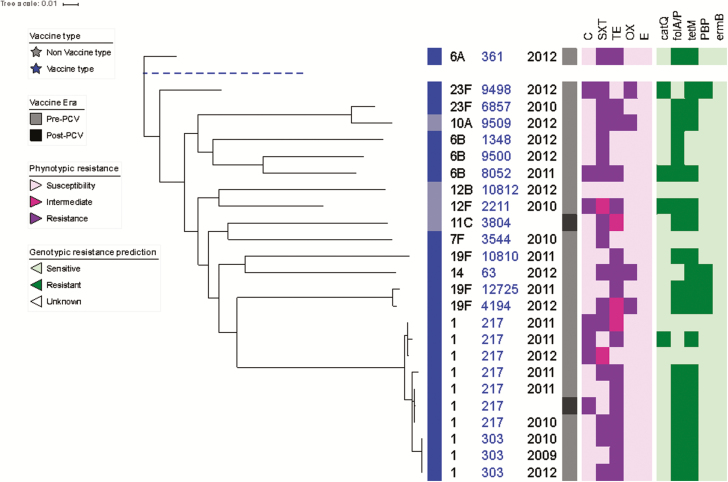
Methods: Cerebrospinal fluid (CSF) specimens from children <5 years old with suspected meningitis were tested to detect vaccine-preventable bacterial pathogens. Confirmatory identification and serotyping/grouping of Streptococcus pneumoniae, N. meningitidis, and H. influenzae were done. Antimicrobial susceptibility testing and whole genome sequencing were performed on S. pneumoniae isolates.
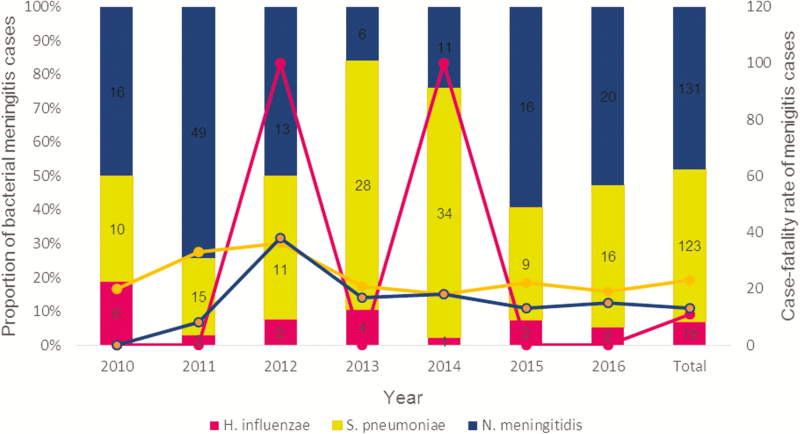
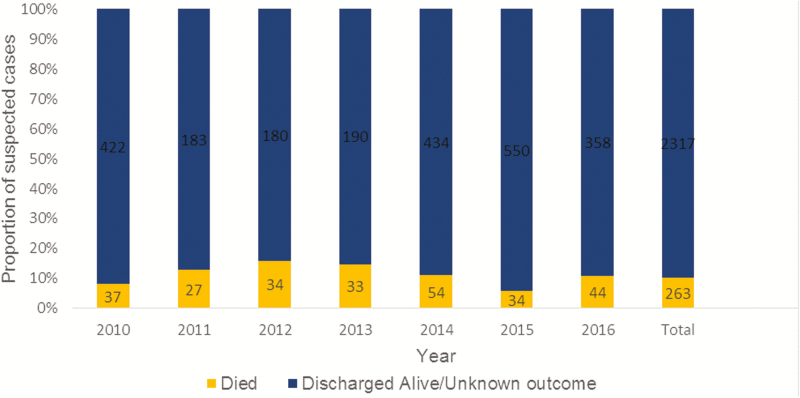
Results: The surveillance included 2580 patients with suspected meningitis, of whom 80.8% (2085/2580) had CSF collected. Bacterial meningitis was confirmed in 273 patients: 48% (131/273) was N. meningitidis, 45% (123/273) S. pneumoniae, and 7% (19/273) H. influenzae. Streptococcus pneumoniae meningitis decreased from 34 in 2014, to 16 in 2016. PCV13 serotypes made up 88% (7/8) of S. pneumoniae meningitis prevaccination and 20% (5/20) postvaccination. Neisseria meningitidis serogroup C (NmC) was responsible for 59% (10/17) of serogrouped N. meningitidis meningitis. Hib caused 67% (2/3) of the H. influenzae meningitis isolates serotyped. Penicillin resistance was found in 16% (4/25) of S. pneumoniae isolates. Sequence type 217 was the most common lineage among S. pneumoniae isolates.
Conclusions: Neisseria meningitidis and S. pneumoniae remain important causes of meningitis in children in Niger. The decline in the numbers of S. pneumoniae meningitis post-PCV13 is encouraging and should continue to be monitored. NmC is the predominant serogroup causing N. meningitidis meningitis.
Keywords: N. meningitidis; S. pneumoniae; Niger; cerebrospinal fluid; meningitis.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Burki T. Meningitis outbreak in Niger is an urgent warning. Lancet Infect Dis 2015; 15:1011. - PubMed
-
- Collard JM, Maman Z, Abani A, et al. Microbiological and epidemiological investigation of the Neisseria meningitidis serogroup A epidemic in Niger in 2009: last wave before the introduction of the serogroup A meningococcal conjugate vaccine? Epidemiol Infect 2011; 139:1656–60. - PubMed
-
- Boisier P, Nicolas P, Djibo S, et al. Meningococcal meningitis: unprecedented incidence of serogroup X-related cases in 2006 in Niger. Clin Infect Dis 2007; 44:657–63. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
