

Pharmacogenomic genotypes define genetic ancestry in patients and enable population-specific genomic implementation
- PMID: 31506565
- PMCID: PMC7184888
- DOI: 10.1038/s41397-019-0095-z
Pharmacogenomic genotypes define genetic ancestry in patients and enable population-specific genomic implementation
Abstract
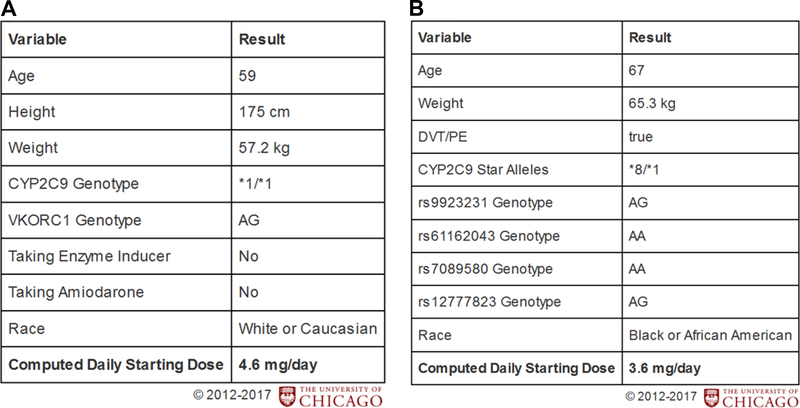
The importance of genetic ancestry characterization is increasing in genomic implementation efforts, and clinical pharmacogenomic guidelines are being published that include population-specific recommendations. Our aim was to test the ability of focused clinical pharmacogenomic SNP panels to estimate individual genetic ancestry (IGA) and implement population-specific pharmacogenomic clinical decision-support (CDS) tools. Principle components and STRUCTURE were utilized to assess differences in genetic composition and estimate IGA among 1572 individuals from 1000 Genomes, two independent cohorts of Caucasians and African Americans (AAs), plus a real-world validation population of patients undergoing pharmacogenomic genotyping. We found that clinical pharmacogenomic SNP panels accurately estimate IGA compared to genome-wide genotyping and identify AAs with ≥70 African ancestry (sensitivity >82%, specificity >80%, PPV >95%, NPV >47%). We also validated a new AA-specific warfarin dosing algorithm for patients with ≥70% African ancestry and implemented it at our institution as a novel CDS tool. Consideration of IGA to develop an institutional CDS tool was accomplished to enable population-specific pharmacogenomic guidance at the point-of-care. These capabilities were immediately applied for guidance of warfarin dosing in AAs versus Caucasians, but also provide a real-world model that can be extended to other populations and drugs as actionable genomic evidence accumulates.
Conflict of interest statement
Conflict of interest
K.D., M.J.R., and P.H.O. are co-inventors on a pending patent application for a Genomic Prescribing System. M.J.R. receives royalties related to
Figures


References
-
- Bachtiar M, Lee CGL. Genetics of Population Differences in Drug Response. Curr Genet Med Rep. 2013;1:162–170.
-
- Jittikoon J, Mahasirimongkol S, Charoenyingwattana A, et al. Comparison of genetic variation in drug ADME-related genes in Thais with Caucasian, African and Asian HapMap populations. J Hum Genet. 2016;61(2):119–127. - PubMed
-
- Wilson JF, Weale ME, Smith AC, et al. Population genetic structure of variable drug response. Nat Genet. 2001;29(3):265–269. - PubMed
-
- Ramos E, Doumatey A, Elkahloun AG, et al. Pharmacogenomics, ancestry and clinical decision making for global populations. Pharmacogenomics J. 2014;14(3):217–222. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
