

MRI-Based Predictors of Hemorrhagic Transformation in Patients With Stroke Treated by Intravenous Thrombolysis
- PMID: 31507511
- PMCID: PMC6719609
- DOI: 10.3389/fneur.2019.00897
MRI-Based Predictors of Hemorrhagic Transformation in Patients With Stroke Treated by Intravenous Thrombolysis
Abstract
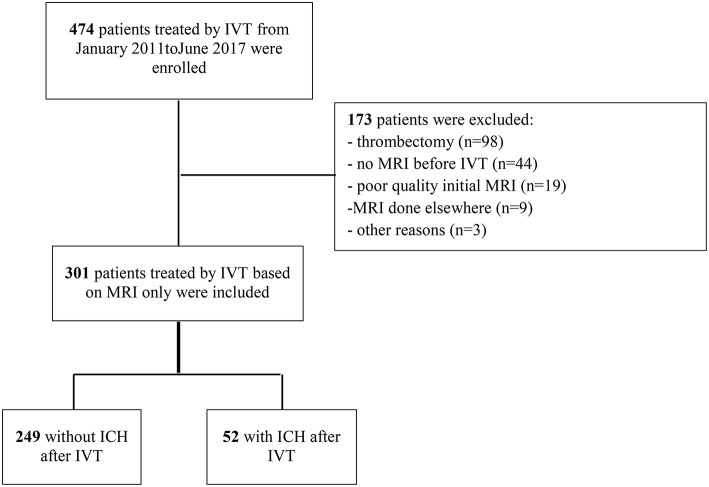
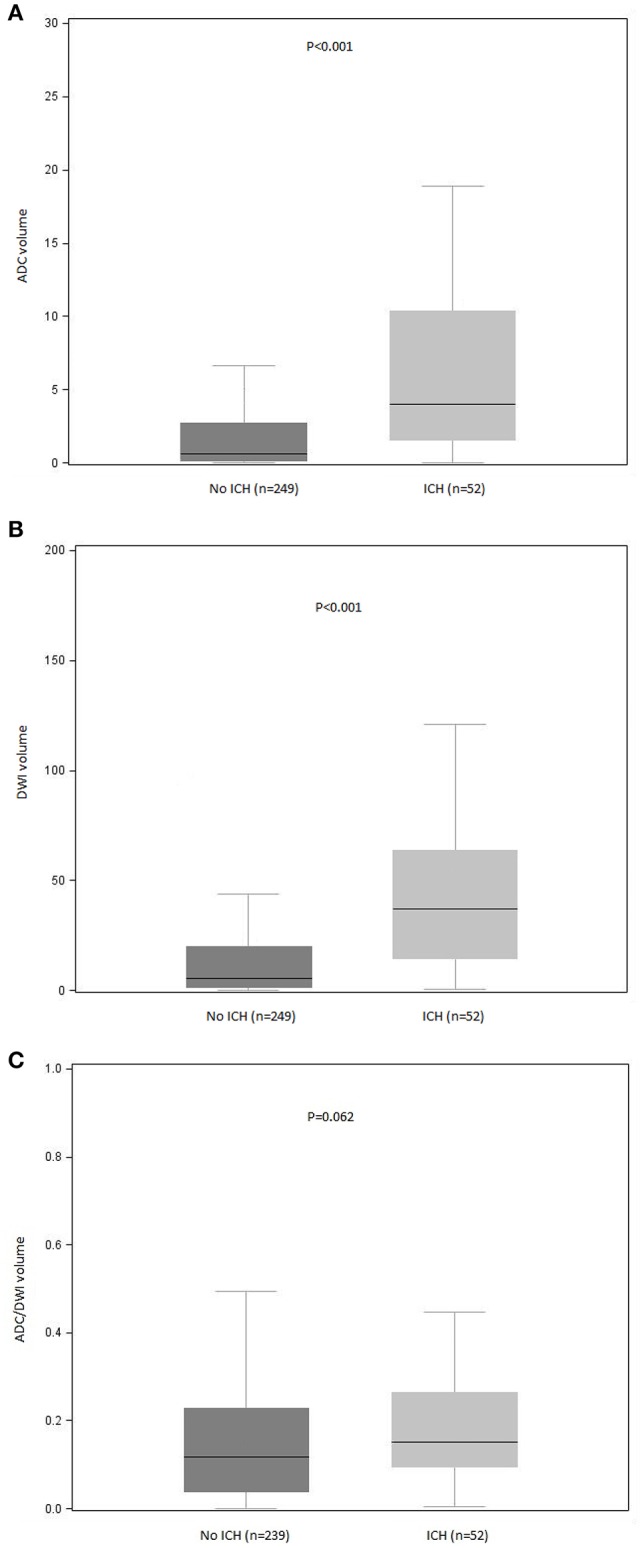
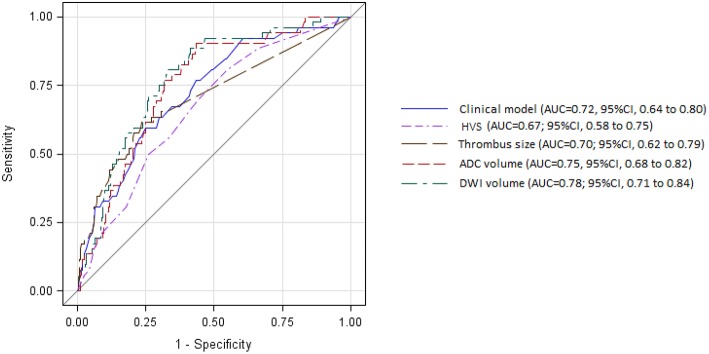
Background: Clinical and biological risk factors for hemorrhagic transformation (HT) after intravenous thrombolysis (IT) have been well-established in several registries. The added value of magnetic resonance imaging (MRI) variables has been studied in small samples, and is controversial. We aimed to assess the added value of MRI variables in HT, beyond that of clinical and biological factors. Methods: We enrolled 474 consecutive patients with brain infarction treated by IT alone at our primary stroke center between January 2011 and August 2017. Baseline demographic, clinical, biological, and imaging characteristics were collected. MRI variables were: brain infarction volume in cm3; parenchymal fluid attenuated inversion recovery (FLAIR) hyperintensity; FLAIR hyperintense vessel signs; number of microbleeds; subcortical white matter hyperintensity; and thrombus length. Results: Overall, 301 patients were included out of 474 (64%). The main causes of exclusion were combined thrombectomy (n = 98) and no MRI before IT (n = 44). In the bivariate analysis, HT was significantly associated with the presence of more FLAIR hyperintense vessel signs, thrombus length (>8 mm), and larger brain infarction volume (diffusion-weighted imaging (DWI) and apparent diffusion coefficient (ADC) < 500 × 10-6 mm2/s). In the multivariable analysis, only brain infarction volume was significantly associated with HT. The discrimination value of the multivariable model, including both the DWI volume and the clinical model (area under the receiver operating characteristic curve, 0.80; 95% confidence interval 0.74-0.86), was improved significantly compared with the model based only on clinical variables (P = 0.012). Conclusions: Brain infarction volume on DWI was the only MRI variable that added value to clinico biological variables for predicting HT after IT.
Keywords: diffusion-weighted imaging; hemorrhage; intravenous thrombolysis; ischemic; magnetic resonance imaging; stroke.
Figures
References
-
- Wahlgren N, Ahmed N, Davalos A, Ford GA, Grond M, Hacke W, et al. . Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): an observational study. Lancet. (2007) 369:275–82. 10.1016/S0140-6736(07)60149-4 - DOI - PubMed
LinkOut - more resources
Full Text Sources