

NK Cells Contribute to the Immune Risk Profile in Kidney Transplant Candidates
- PMID: 31507586
- PMCID: PMC6716214
- DOI: 10.3389/fimmu.2019.01890
NK Cells Contribute to the Immune Risk Profile in Kidney Transplant Candidates
Abstract
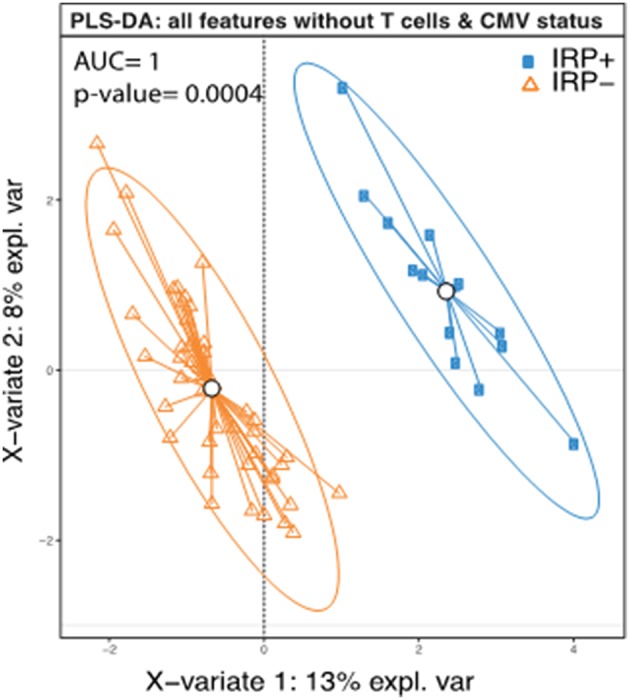
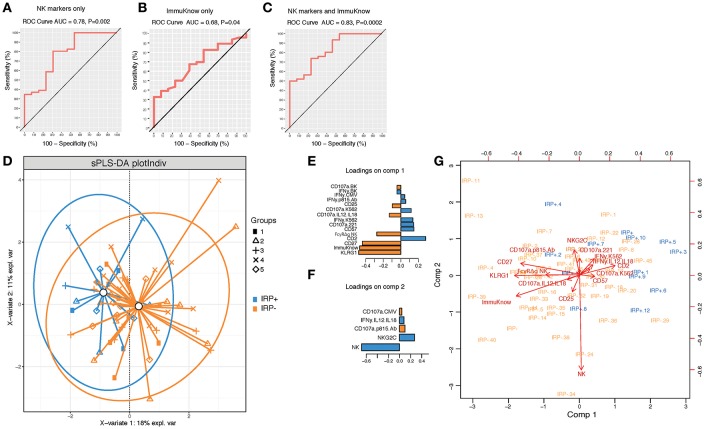
Background: A previously proposed immune risk profile (IRP), based on T cell phenotype and CMV serotype, is associated with mortality in the elderly and increased infections post-kidney transplant. To evaluate if NK cells contribute to the IRP and if the IRP can be predicted by a clinical T cell functional assays, we conducted a cross sectional study in renal transplant candidates to determine the incidence of IRP and its association with specific NK cell characteristics and ImmuKnow® value. Material and Methods: Sixty five subjects were enrolled in 5 cohorts designated by age and dialysis status. We determined T and NK cell phenotypes by flow cytometry and analyzed multiple factors contributing to IRP. Results: We identified 14 IRP+ [CMV seropositivity and CD4/CD8 ratio < 1 or being in the highest quintile of CD8+ senescent (28CD-/CD57+) T cells] individuals equally divided amongst the cohorts. Multivariable linear regression revealed a distinct IRP+ group. Age and dialysis status did not predict immune senescence in kidney transplant candidates. NK cell features alone could discriminate IRP- and IRP+ patients, suggesting that NK cells significantly contribute to the overall immune status in kidney transplant candidates and that a combined T and NK cell phenotyping can provide a more detailed IRP definition. ImmuKnow® value was negatively correlated to age and significantly lower in IRP+ patients and predicts IRP when used alone or in combination with NK cell features. Conclusion: NK cells contribute to overall immune senescence in kidney transplant candidates.
Keywords: BK virus; NK cells; dialysis; end stage renal disease; immune risk profile; immune senescence; kidney transplant.
Figures
Similar articles
-
Independent skewing of the T cell and NK cell compartments associated with cytomegalovirus infection suggests division of labor between innate and adaptive immunity.Age (Dordr). 2014 Apr;36(2):571-82. doi: 10.1007/s11357-013-9587-y. Epub 2013 Sep 25. Age (Dordr). 2014. PMID: 24065293 Free PMC article.
-
CMV drives the expansion of highly functional memory T cells expressing NK-cell receptors in renal transplant recipients.Eur J Immunol. 2017 Aug;47(8):1324-1334. doi: 10.1002/eji.201747018. Epub 2017 Jul 3. Eur J Immunol. 2017. PMID: 28586095
-
Pre-transplant end-stage renal disease-related immune risk profile in kidney transplant recipients predicts post-transplant infections.Transpl Infect Dis. 2016 Jun;18(3):415-22. doi: 10.1111/tid.12534. Epub 2016 May 21. Transpl Infect Dis. 2016. PMID: 27027787
-
Role of CMV in immune senescence.Virus Res. 2011 May;157(2):175-9. doi: 10.1016/j.virusres.2010.09.010. Epub 2010 Oct 1. Virus Res. 2011. PMID: 20869407 Review.
-
Molecular characterization of HCMV-specific immune responses: Parallels between CD8(+) T cells, CD4(+) T cells, and NK cells.Eur J Immunol. 2015 Sep;45(9):2433-45. doi: 10.1002/eji.201545495. Epub 2015 Aug 24. Eur J Immunol. 2015. PMID: 26228786 Review.
Cited by
-
Association of IL-15 and IP-10 Serum Levels with Cytomegalovirus Infection, CMV Viral Load and Cyclosporine Level after Kidney Transplantation.Rep Biochem Mol Biol. 2021 Jul;10(2):216-223. doi: 10.52547/rbmb.10.2.216. Rep Biochem Mol Biol. 2021. PMID: 34604411 Free PMC article.
-
Perirenal Adipose Tissue Displays an Age-Dependent Inflammatory Signature Associated With Early Graft Dysfunction of Marginal Kidney Transplants.Front Immunol. 2020 Mar 17;11:445. doi: 10.3389/fimmu.2020.00445. eCollection 2020. Front Immunol. 2020. PMID: 32256495 Free PMC article.
References
-
- Matsumoto Y, Shinzato T, Amano I, Takai I, Kimura Y, Morita H, et al. . Relationship between susceptibility to apoptosis and Fas expression in peripheral blood T cells from uremic patients: a possible mechanism for lymphopenia in chronic renal failure. Biochem Biophys Res Commun. (1995) 215:98–105. 10.1006/bbrc.1995.2438 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials