

RELIABILITY OF THE CORTICOTROPIN RELEASING HORMONE STIMULATION TEST FOR DIFFERENTIATING BETWEEN ACTH DEPENDENT AND INDEPENDENT CUSHING SYNDROME
- PMID: 31508176
- PMCID: PMC6711639
- DOI: 10.4183/aeb.2019.195
RELIABILITY OF THE CORTICOTROPIN RELEASING HORMONE STIMULATION TEST FOR DIFFERENTIATING BETWEEN ACTH DEPENDENT AND INDEPENDENT CUSHING SYNDROME
Abstract
Context: It is a challenge to determine the origin of Cushing syndrome (CS), especially in patients with low-normal adrenocorticotropic hormone (ACTH) concentrations.
Objective: To evaluate the reliability of the corticotropin-releasing hormone (CRH) stimulation test in patients with CS whose origin of disease was not clearly identified using ACTH values, the high-dose dexamethasone suppression test (HDDST), and imaging in a single tertiary referral center.
Design and methods: Twenty-one patients with CS who were admitted to the endocrinology-metabolism clinic between 2004 and 2016 whose ACTH concentrations were 5-20 pg/mL and needed CRH stimulation test were retrospectively assessed.
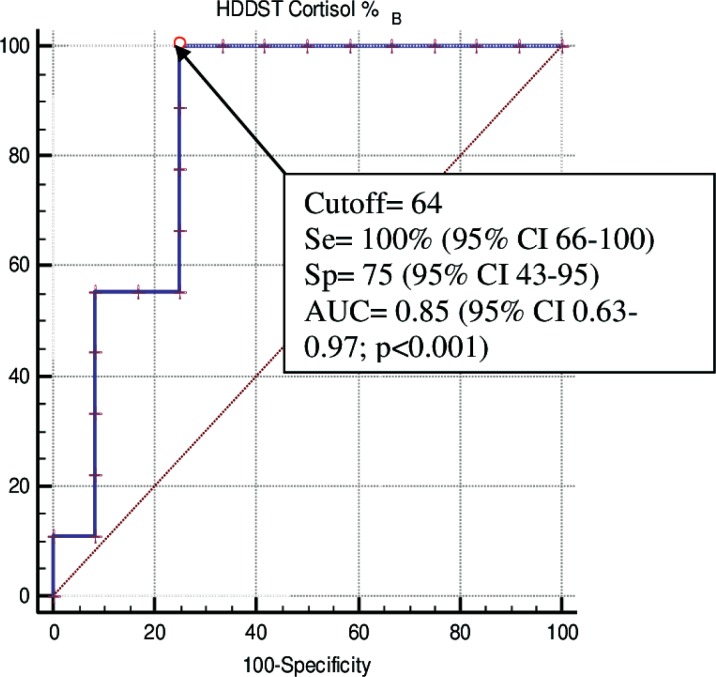
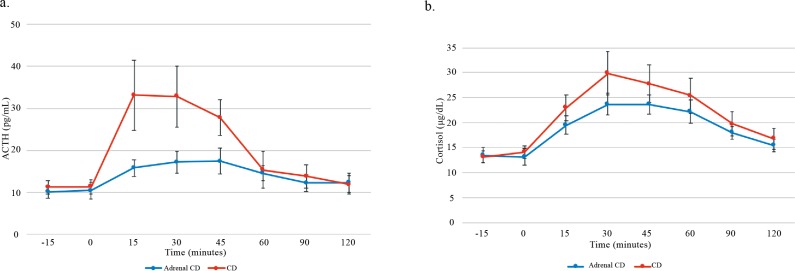
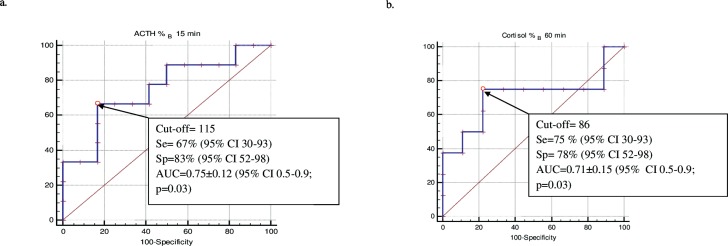
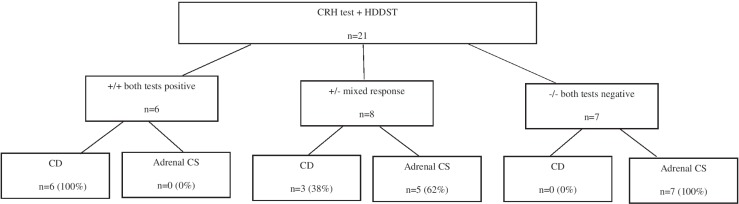
Results: Nine out of 21 patients were diagnosed as having Cushing's disease (CD) and 12/21 had adrenal CS. The CRH stimulation test had a sensitivity and specificity of 100% and 8%, and positive and negative predictive values of 100% and 45% according to the current diagnostic criteria, respectively. An increase in ACTH ≥115% at 15 minutes and cortisol ≥86% at 60 minutes after CRH were associated with the highest likelihood ratio. The sensitivity and specificity of ACTH was 67% and 83% (AUC=0.75±0.12, 95% CI: [0.5-0.9]; p=0.03), and for cortisol it was 75% and 78% (AUC=0.71±0.15, 95% CI: [0.5-0.9]; p=0.03). Cortisol suppression of more than 64% from basal level in the HDDST suggested CD with the highest likelihood ratio. When these cut-off values were used together, both tests were negative in the patients with CD.
Conclusion: The CRH stimulation test has low specificity to localize CS in patients with ACTH concentrations of 5-20 pg/mL according to the current diagnostic criteria. Different diagnostic criteria may be used in the CRH stimulation test and also in the HDDST in this group of patients.
Keywords: ACTH; CRH stimulation test; Cushing’s syndrome.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Bertagna X, Guignat L, Groussin L, Bertherat J. Cushing’s disease. Best Pract Res Clin Endocrinol Metab. 2009;23(5):607–623. - PubMed
-
- Mantero F, Terzolo M, Arnaldi G, Osella G, Masini AM, Alì A, Giovagnetti M, Opocher G, Angeli A, Study Group on Adrenal Tumors of the Italian Society of Endocrinology A survey on adrenal incidentaloma in Italy. J Clin Endocrinol Metab. 2000;85(2):637–644. - PubMed
-
- Lindsay JR, Nieman LK. Differential diagnosis and imaging in Cushing’s syndrome. Endocrinol Metab Clin North Am. 2005;34(2):403–421. - PubMed
-
- Juszczak A, Grossman A. The management of Cushing’s disease - from investigation to treatment. Endokrynol Pol. 2013;64(2):166–174. - PubMed
-
- Newell-Price J, Bertagna X, Grossman AB, Nieman LK. Cushing’s syndrome. Lancet. 2006;367(9522):1605–1617. - PubMed
LinkOut - more resources
Full Text Sources