

Uremic leontiasis ossea due to secondary hyperparathyroidism complicated by vitamin C deficiency in a non-adherent chronic hemodialysis patient: A case report
- PMID: 31508269
- PMCID: PMC6734544
- DOI: 10.5414/CNCS109788
Uremic leontiasis ossea due to secondary hyperparathyroidism complicated by vitamin C deficiency in a non-adherent chronic hemodialysis patient: A case report
Abstract
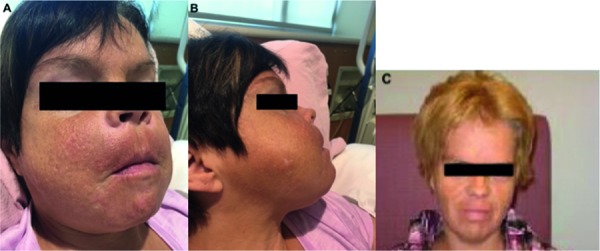
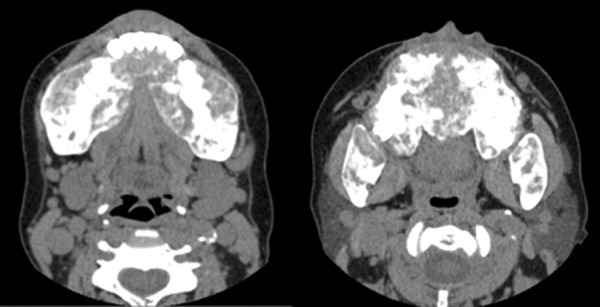
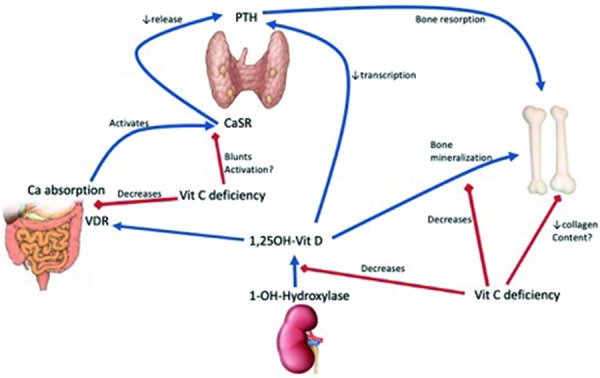
Non-adherence to medical therapy in patients with end-stage kidney disease (ESKD) can lead to severe metabolic derangements rarely seen in the current medical era. Such complications may take the form of secondary hyperparathyroidism (HPT) leading to rare manifestations of bone mineral disease, and profound vitamin C deficiency from poor nutrition combined with removal of water-soluble vitamins during dialysis. Secondary HPT causes renal osteodystrophy which can lead to diffuse enlargement of the facial skeleton and morphological changes suggestive of leontiasis ossea. We report a 36-year-old, non-adherent woman on chronic dialysis for over 10 years who developed progressive, diffuse facial bone enlargement in the context of years of extreme HPT and newly diagnosed severe vitamin C deficiency. Imaging revealed diffuse hypertrophy of the maxillary and mandibular bones. Histopathology showed extensive fibro-osseous proliferation without evidence of Brown tumor, suggestive of uremic leontiasis ossea. In this report, we discuss the orofacial manifestations of secondary HPT and the possible potentiating role of vitamin C deficiency on the development of renal osteodystrophy through altered vitamin D metabolism. Non-adherent patients on chronic dialysis should be evaluated for vitamin C deficiency, and the development of uremic leontiasis ossea should be considered when such patients present with distortion of facial features in the context of severe secondary HPT.
Keywords: end-stage kidney disease; hyperparathyroidism; leontiasis ossea; non-adherence; renal osteodystrophy; vitamin C deficiency.
Figures
Similar articles
-
Uremic Leontiasis Ossea in a Patient With End-Stage Renal Disease in Hemodialysis.Cureus. 2020 Oct 20;12(10):e11060. doi: 10.7759/cureus.11060. Cureus. 2020. PMID: 33224656 Free PMC article.
-
Uremic leontiasis ossea: distinctive imaging features allow differentiation from other clinical causes of leontiasis ossea.Radiol Case Rep. 2021 Dec 16;17(3):553-557. doi: 10.1016/j.radcr.2021.11.061. eCollection 2022 Mar. Radiol Case Rep. 2021. PMID: 34987683 Free PMC article.
-
Uremic leontiasis ossea, a rare presentation of severe renal osteodystrophy secondary to hyperparathyroidism.J Stomatol Oral Maxillofac Surg. 2018 Feb;119(1):56-60. doi: 10.1016/j.jormas.2017.10.006. Epub 2017 Oct 14. J Stomatol Oral Maxillofac Surg. 2018. PMID: 29037869
-
1alpha(OH)D3 One-alpha-hydroxy-cholecalciferol--an active vitamin D analog. Clinical studies on prophylaxis and treatment of secondary hyperparathyroidism in uremic patients on chronic dialysis.Dan Med Bull. 2008 Nov;55(4):186-210. Dan Med Bull. 2008. PMID: 19232159 Review.
-
Uremic Leontiasis Ossea: Theoretical Concepts and Practical Considerations.Saudi J Kidney Dis Transpl. 2022 Sep 1;33(5):702-715. doi: 10.4103/1319-2442.389430. Epub 2023 Nov 7. Saudi J Kidney Dis Transpl. 2022. PMID: 37955462 Review.
Cited by
-
Two Faces of Vitamin C in Hemodialysis Patients: Relation to Oxidative Stress and Inflammation.Nutrients. 2021 Feb 27;13(3):791. doi: 10.3390/nu13030791. Nutrients. 2021. PMID: 33673687 Free PMC article. Review.
-
Uremic Leontiasis Ossea in a Patient With End-Stage Renal Disease in Hemodialysis.Cureus. 2020 Oct 20;12(10):e11060. doi: 10.7759/cureus.11060. Cureus. 2020. PMID: 33224656 Free PMC article.
-
Uremic leontiasis ossea: distinctive imaging features allow differentiation from other clinical causes of leontiasis ossea.Radiol Case Rep. 2021 Dec 16;17(3):553-557. doi: 10.1016/j.radcr.2021.11.061. eCollection 2022 Mar. Radiol Case Rep. 2021. PMID: 34987683 Free PMC article.
References
-
- Descombes E Hanck AB Fellay G Water soluble vitamins in chronic hemodialysis patients and need for supplementation. Kidney Int. 1993; 43: 1319–1328. - PubMed
-
- Singer R Rhodes HC Chin G Kulkarni H Ferrari P High prevalence of ascorbate deficiency in an Australian peritoneal dialysis population. Nephrology (Carlton). 2008; 13: 17–22. - PubMed
-
- Richter A Kuhlmann MK Seibert E Kotanko P Levin NW Handelman GJ Vitamin C deficiency and secondary hyperparathyroidism in chronic haemodialysis patients. Nephrol Dial Transplant. 2008; 23: 2058–2063. - PubMed
-
- Attallah N Osman-Malik Y Frinak S Besarab A Effect of intravenous ascorbic acid in hemodialysis patients with EPO-hyporesponsive anemia and hyperferritinemia. Am J Kidney Dis. 2006; 47: 644–654. - PubMed
-
- Deicher R Hörl WH Vitamin C in chronic kidney disease and hemodialysis patients. Kidney Blood Press Res. 2003; 26: 100–106. - PubMed
Publication types
LinkOut - more resources
Full Text Sources