

Changes of median nerve conduction, cross-sectional area and mobility by radioulnar wrist compression intervention in patients with carpal tunnel syndrome
- PMID: 31508303
- PMCID: PMC6718919
- DOI: 10.1016/j.jot.2019.01.002
Changes of median nerve conduction, cross-sectional area and mobility by radioulnar wrist compression intervention in patients with carpal tunnel syndrome
Abstract
Background: Owing to the compressive nature of the neuropathy, patients with carpal tunnel syndrome (CTS) have prolonged distal motor latency (DML), sensory nerve latency (SNL), median nerve swelling and restricted median nerve mobility. The purpose of this study was to noninvasively augment carpal tunnel space using radioulnar wrist compression (RWC) and evaluate its effects on median nerve pathological properties in patients with CTS. It was hypothesized that the RWC intervention would reduce the median nerve DML, SNL and cross-sectional area (CSA) and enhance longitudinal median nerve mobility in patients. with CTS.
Methods: Eleven patients diagnosed with CTS participated in this study. A portable RWC intervention splint was developed to apply 10 N of compressive force across the wrist. Three daily sessions of RWC were performed over 4 weeks of intervention (15 min per session, 45 min per day, 7 days per week). Each 15-min session consisted of three 5-min blocks of RWC, with a 1-min rest in between consecutive blocks. Patients were evaluated at Week 0 (baseline), Week 2 (mid-intervention) and Week 4 (end of intervention). DML and SNL of the median nerve were evaluated using established nerve conduction study techniques. Median nerve CSA at the distal wrist crease was obtained by ultrasound imaging. Median nerve motion associated with finger flexion/extension was captured by dynamic ultrasound imaging and quantified using a speckle cross-correlation algorithm. Finger flexion/extension was recorded using an electrogoniometer. The slope of the regressed linear equation of median nerve displacement as a function of finger flexion angle was used to quantify nerve mobility.
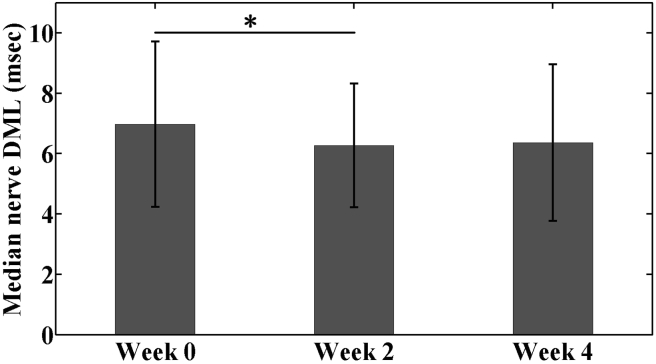
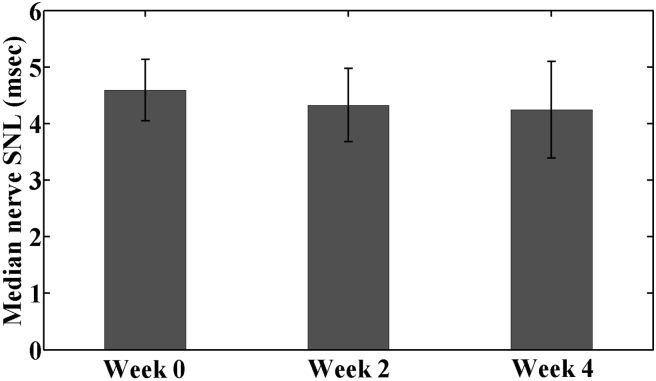
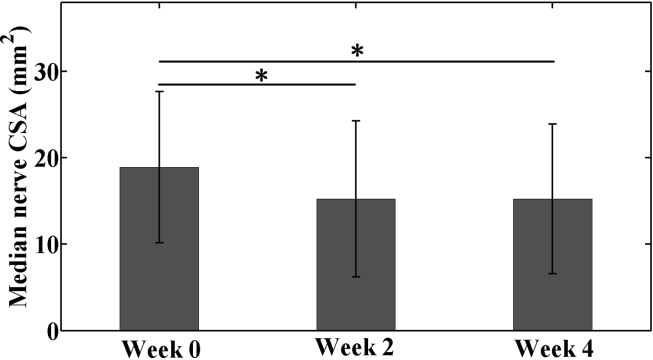
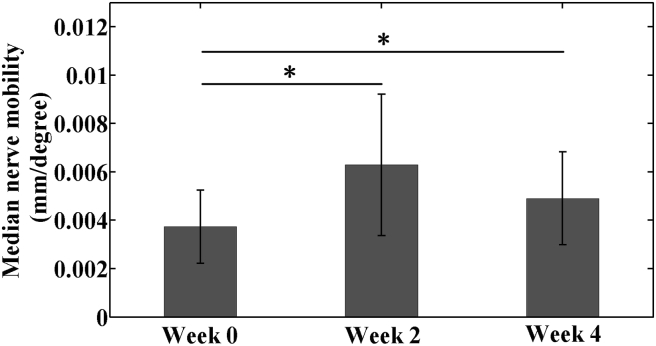
Results: Patients with CTS showed significantly decreased DML (p = 0.048) and median nerve CSA (p < 0.001) and increased nerve mobility (p < 0.001) at mid-intervention compared to baseline. However, DML, CSA and mobility of the median nerve did not differ significantly between Weeks 2 and 4 (p = 0.574, 1.00 and 0.139, respectively). Median nerve SNL was not significantly affected throughout the 4-week intervention (p = 0.330 for Week 0 vs. 2; p = 1.00 for Week 2 vs. 4).
Conclusion: This study revealed that RWC intervention with 10-N force applied to the wrist in the radioulnar direction could restore impaired neurophysiological and biomechanical functions of the median nerve. The beneficial effects of RWC intervention for the median nerve were in evidence after a relatively short period of two weeks. These functional improvements could be explained by intermittent decompression of the median nerve via RWC-induced augmentation of the carpal arch.
The translational potential of this article: Biomechanically manipulating the carpal tunnel by RWC decompresses the median nerve and has the potential to become an alternative treatment for CTS.
Keywords: Carpal tunnel syndrome; Cross-sectional area; Median nerve; Mobility; Nerve conduction; Radioulnar wrist compression.
Figures
Similar articles
-
Dexamethasone versus Hyaluronidase as an Adjuvant to Local Anesthetics in the Ultrasound-guided Hydrodissection of the Median Nerve for the Treatment of Carpal Tunnel Syndrome Patients.Anesth Essays Res. 2019 Jul-Sep;13(3):417-422. doi: 10.4103/aer.AER_104_19. Anesth Essays Res. 2019. PMID: 31602055 Free PMC article.
-
The effects of wrist position and radioulnar wrist compression on median nerve longitudinal mobility.Clin Biomech (Bristol). 2022 Oct;99:105754. doi: 10.1016/j.clinbiomech.2022.105754. Epub 2022 Aug 29. Clin Biomech (Bristol). 2022. PMID: 36057239
-
Enhancement in median nerve mobility during radioulnar wrist compression in carpal tunnel syndrome patients.Clin Biomech (Bristol). 2018 Dec;60:83-88. doi: 10.1016/j.clinbiomech.2018.10.017. Epub 2018 Oct 12. Clin Biomech (Bristol). 2018. PMID: 30336369 Free PMC article.
-
Grey-scale sonography and sonoelastography for diagnosing carpal tunnel syndrome.World J Radiol. 2016 Mar 28;8(3):281-7. doi: 10.4329/wjr.v8.i3.281. World J Radiol. 2016. PMID: 27027498 Free PMC article. Review.
-
Meta-analysis on effects of lymphatic drainage techniques in the management of carpal tunnel syndrome.J Orthop Surg Res. 2025 May 20;20(1):491. doi: 10.1186/s13018-025-05887-w. J Orthop Surg Res. 2025. PMID: 40394623 Free PMC article.
Cited by
-
Carpal arch space increased by volar force applied to the skin surface above the carpal tunnel.Clin Biomech (Bristol). 2023 Feb;102:105888. doi: 10.1016/j.clinbiomech.2023.105888. Epub 2023 Jan 11. Clin Biomech (Bristol). 2023. PMID: 36640747 Free PMC article.
-
Carpal tunnel mechanics and its relevance to carpal tunnel syndrome.Hum Mov Sci. 2023 Feb;87:103044. doi: 10.1016/j.humov.2022.103044. Epub 2022 Nov 25. Hum Mov Sci. 2023. PMID: 36442295 Free PMC article. Review.
-
The Morphological and Dynamic Changes of Ultrasound in the Evaluation of Effects of Oral Steroids Treatment for Patients with Carpal Tunnel Syndrome.Diagnostics (Basel). 2021 Jul 26;11(8):1336. doi: 10.3390/diagnostics11081336. Diagnostics (Basel). 2021. PMID: 34441271 Free PMC article.
-
The morphology of a smartphonopathic hand - smartphone use and the median nerve cross-sectional area.Pak J Med Sci. 2025 Jan;41(1):200-204. doi: 10.12669/pjms.41.1.9958. Pak J Med Sci. 2025. PMID: 39867807 Free PMC article.
-
Ultrasound and elastography role in pre- and post-operative evaluation of median neuropathy in patients with carpal tunnel syndrome.Front Neurol. 2022 Dec 16;13:1079737. doi: 10.3389/fneur.2022.1079737. eCollection 2022. Front Neurol. 2022. PMID: 36588903 Free PMC article.
References
-
- Atroshi I., Gummesson C., Johnsson R., Ornstein E., Ranstam J., Rosén I. Prevalence of carpal tunnel syndrome in a general population. J Am Med Assoc. 1999;282(2):153–158. - PubMed
-
- Lluch A.L. Thickening of the synovium of the digital flexor tendons: cause or consequence of the carpal tunnel syndrome? J Hand Surg. 1992;17(2):209–211. - PubMed
-
- Jablecki C.K., Andary C.M.T., So Y.T., Wilkins D.E., Williams F.H. Literature review of the usefulness of nerve conduction studies and electromyography for the evaluation of patients with carpal tunnel syndrome. Muscle Nerve. 1993;16(12):1392–1414. - PubMed
-
- De Krom M.C.T.F.M., Knipschild P.G., Spaans F., Kester A.D.M. Efficacy of provocative tests for diagnosis of carpal tunnel syndrome. Lancet. 1990;335(8686):393–395. - PubMed
-
- De Lean J. Transcarpal median sensory conduction: detection of latent abnormalities in mild carpal tunnel syndrome. Can J Neurol Sci. 1988;15(4):388–393. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
