Masticatory muscle tendon-aponeurosis hyperplasia accompanied by limited mouth opening
- PMID: 31508348
- PMCID: PMC6728625
- DOI: 10.5125/jkaoms.2019.45.4.174
Masticatory muscle tendon-aponeurosis hyperplasia accompanied by limited mouth opening
Abstract
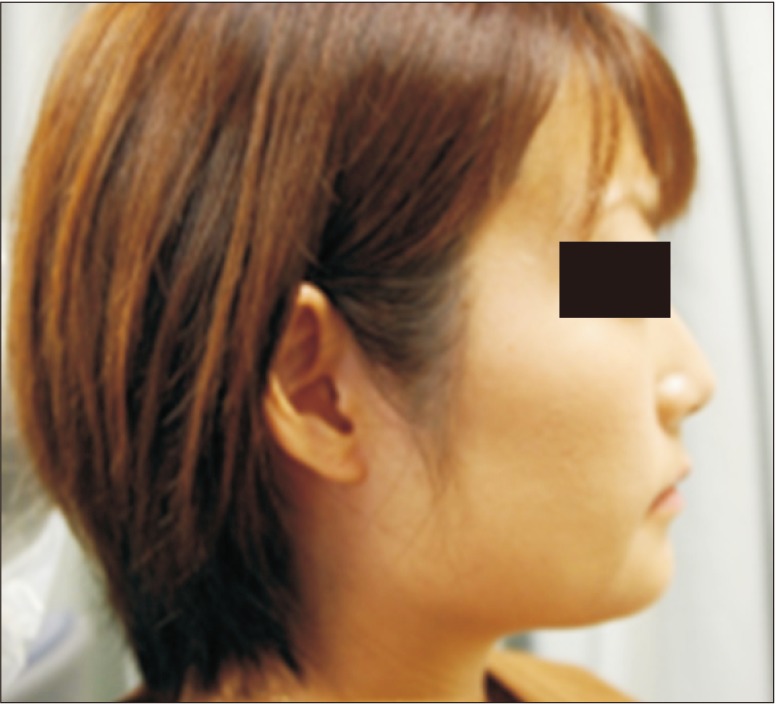
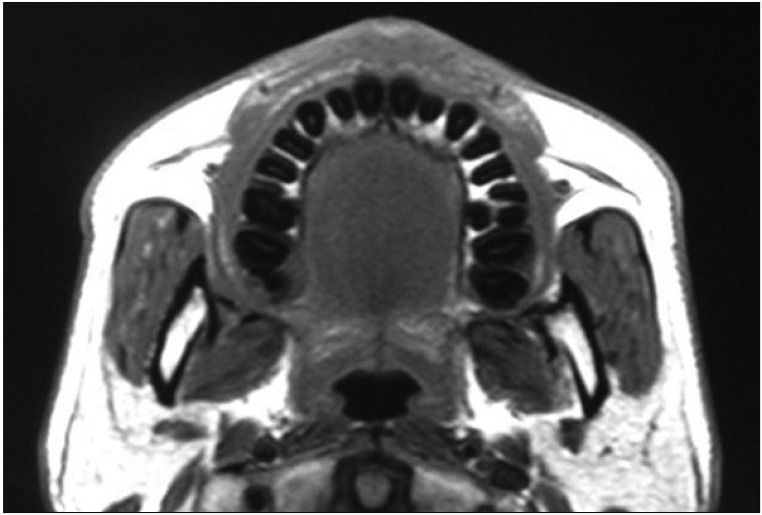
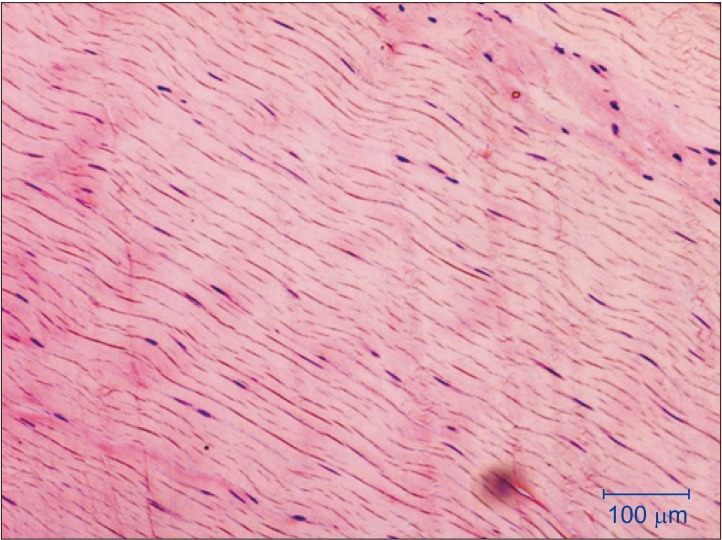
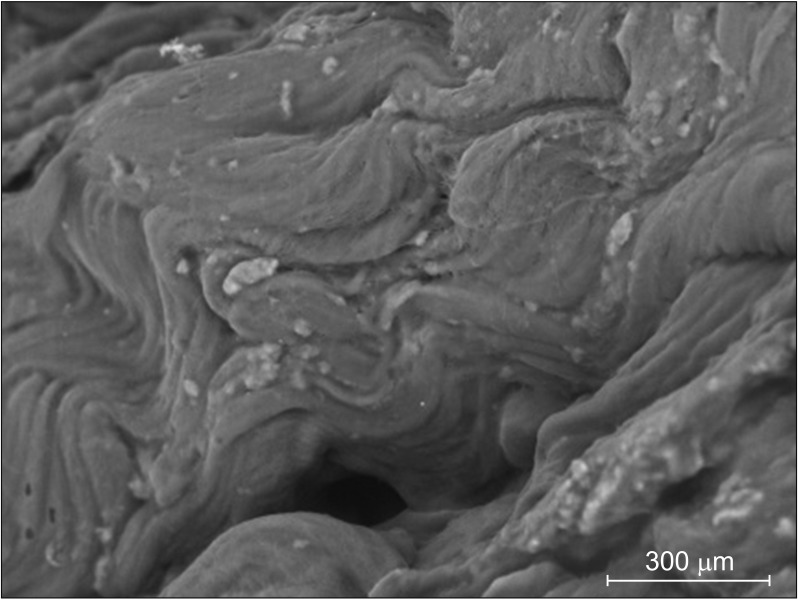
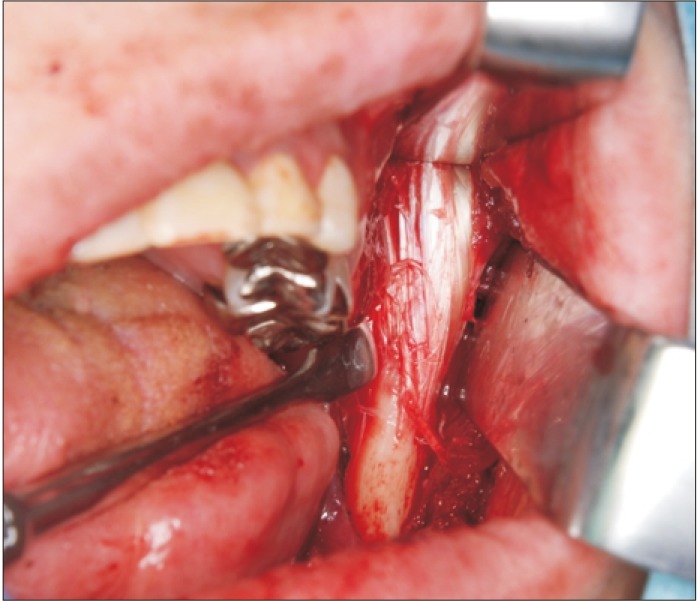
Patients with masticatory muscle tendon-aponeurosis hyperplasia (MMTAH) experience limited mouth opening due to restricted muscle extension. Hyperplastic aponeurosis and tendons lead to the restriction of muscle extension. The criteria for the diagnosis of MMTAH are limited mouth opening that progresses very slowly from adolescence, intraoral palpation reveals a hard cord-like structure along the overhang of the anterior border of the masseter muscle on maximum mouth opening, and a square mandible. Conservative treatment, including pharmacotherapy, occlusal splint and physical therapy are ineffective. The standard therapy is surgical treatment, such as anterior partial aponeurectomy of the masseter muscle and coronoidectomy. The long-term results are very satisfying.
Keywords: Aponeurosis; Limited mouth opening; Masticatory muscle; Tendon.
Conflict of interest statement
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Figures



Similar articles
-
Limited mouth opening with a square mandible configuration: a case of masticatory muscle tendon-aponeurosis hyperplasia.J Surg Case Rep. 2015 Mar 13;2015(3):rjv020. doi: 10.1093/jscr/rjv020. J Surg Case Rep. 2015. PMID: 25770956 Free PMC article.
-
Long-term results of surgical therapy for masticatory muscle tendon-aponeurosis hyperplasia accompanied by limited mouth opening.Int J Oral Maxillofac Surg. 2009 Nov;38(11):1143-7. doi: 10.1016/j.ijom.2009.07.002. Epub 2009 Aug 13. Int J Oral Maxillofac Surg. 2009. PMID: 19682860
-
Masticatory muscle tendon-aponeurosis hyperplasia diagnosed as temporomandibular joint disorder: A case report and review of literature.Int J Surg Case Rep. 2021 Jan;78:120-125. doi: 10.1016/j.ijscr.2020.11.150. Epub 2020 Dec 2. Int J Surg Case Rep. 2021. PMID: 33340978 Free PMC article.
-
Masticatory muscle tendon-aponeurosis hyperplasia: A new clinical entity of limited mouth opening.Jpn Dent Sci Rev. 2016 May;52(2):41-48. doi: 10.1016/j.jdsr.2015.11.001. Epub 2015 Dec 9. Jpn Dent Sci Rev. 2016. PMID: 28408955 Free PMC article. Review.
-
Direct-indirect heat-cured occlusal splint fabrication for a patient with limited mouth opening.Compend Contin Educ Dent. 2000 Feb;21(2):127-32, 134; quiz 136. Compend Contin Educ Dent. 2000. PMID: 11199693 Review.
Cited by
-
Masticatory muscle tendon-aponeurosis hyperplasia that was initially misdiagnosed for polymyositis: a case report and review of the literature.Maxillofac Plast Reconstr Surg. 2023 May 1;45(1):18. doi: 10.1186/s40902-023-00386-6. Maxillofac Plast Reconstr Surg. 2023. PMID: 37126217 Free PMC article.
-
The Usefulness of Mandibular Anglectomy in Patients With Masticatory Muscle Tendon-Aponeurosis Hyperplasia: A Preliminary Single-Center Survey.Cureus. 2024 Dec 2;16(12):e74994. doi: 10.7759/cureus.74994. eCollection 2024 Dec. Cureus. 2024. PMID: 39749059 Free PMC article.
References
-
- Dhanrajani PJ, Jonaidel O. Trismus: aetiology, differential diagnosis and treatment. Dent Update. 2002;29:88–92. 94. - PubMed
-
- Satheeshkumar PS, Mohan MP, Jacob J. Restricted mouth opening and trismus in oral oncology. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;117:709–715. - PubMed
-
- Inoue N, Yamaguchi T, Satou J, Satou C, Minowa K, Iizuka T. A case of restricted mandibular movement resulting from hyperplasia of the masseter muscle aponeurosis. Jpn J Oral Maxillofac Surg. 2000;46:307–309.
-
- Murakami K, Yokoe Y, Yasuda S, Tsuboi Y, Iizuka T. Prolonged mandibular hypomobility patient with a “square mandible” configuration with coronoid process and angle hyperplasia. Cranio. 2000;18:113–119. - PubMed
-
- Beckers HL. Masseteric muscle hypertrophy and its intraoral surgical correction. J Maxillofac Surg. 1977;5:28–35. - PubMed