

Conventional echocardiographic parameters or three-dimensional echocardiography to evaluate right ventricular function in percutaneous edge-to-edge mitral valve repair (PMVR)
- PMID: 31508480
- PMCID: PMC6723083
- DOI: 10.1016/j.ijcha.2019.100413
Conventional echocardiographic parameters or three-dimensional echocardiography to evaluate right ventricular function in percutaneous edge-to-edge mitral valve repair (PMVR)
Abstract
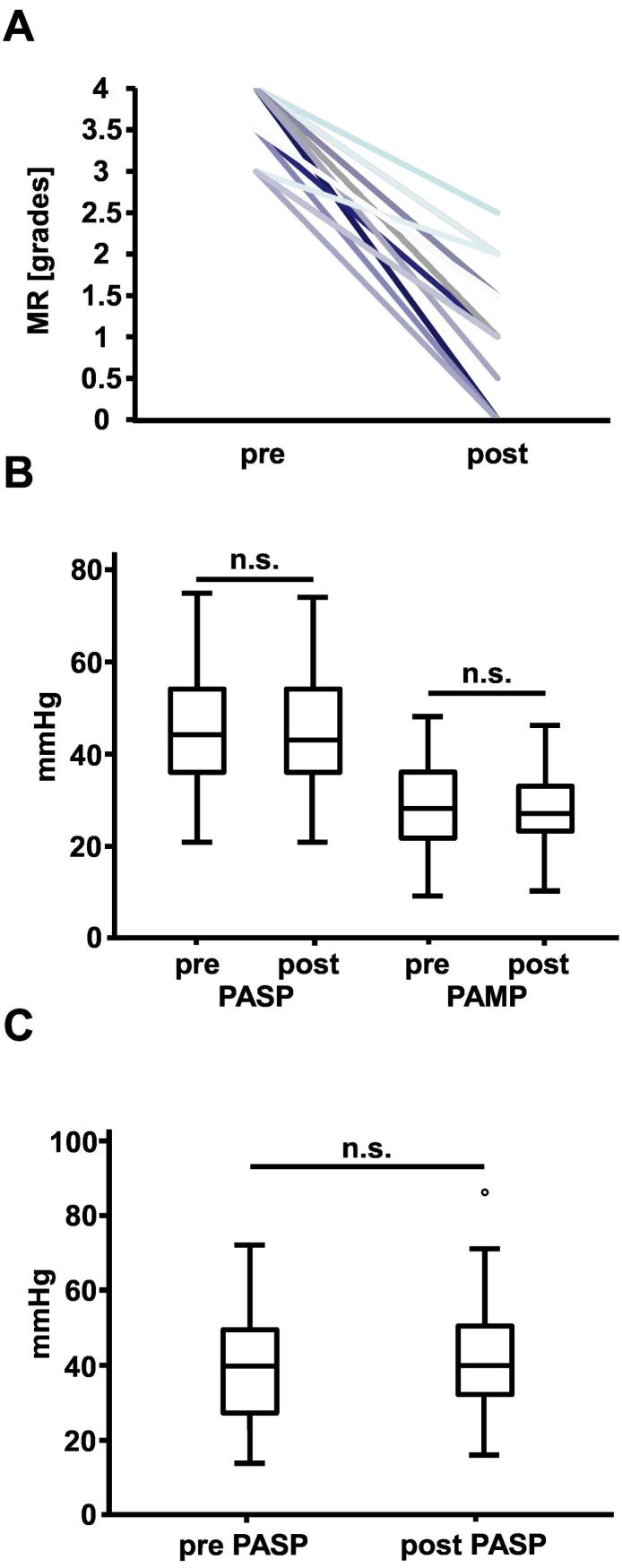
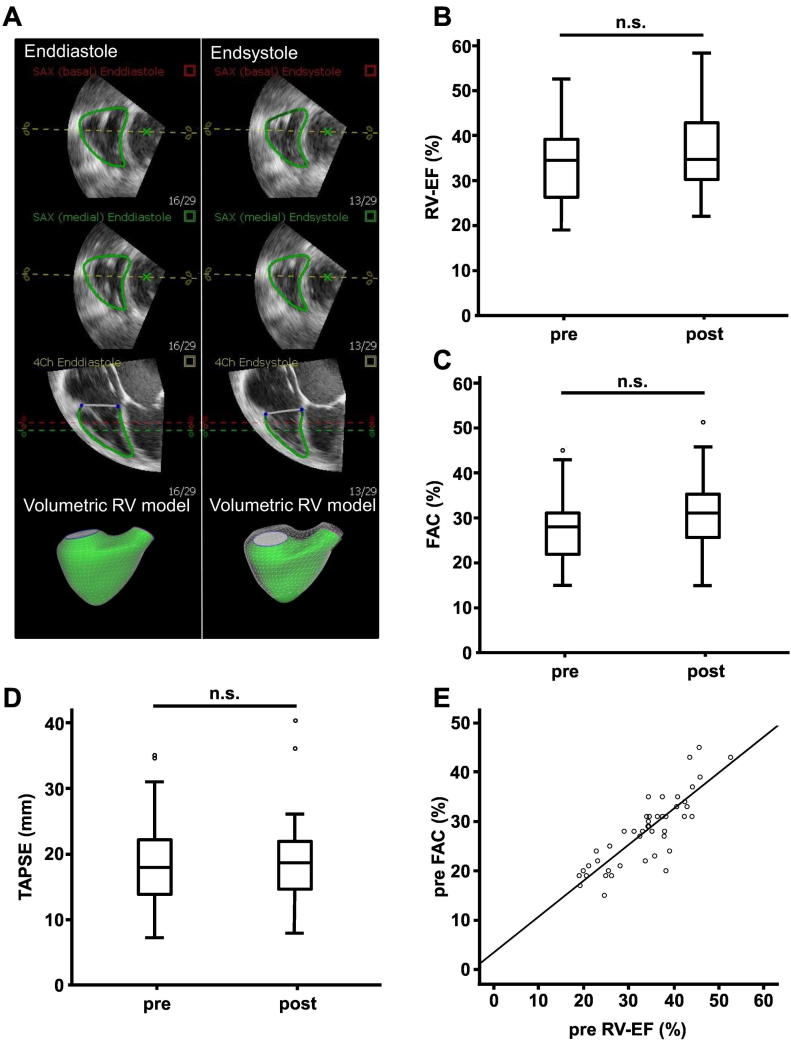
Introduction: In this study, we evaluated right ventricular (RV) function before and after percutaneous mitral valve repair (PMVR) using conventional echocardiographic parameters and novel 3DE data sets acquired prior to and directly after the procedure.
Patients and methods: Observational study on 45 patients undergoing PMVR at an university hospital.
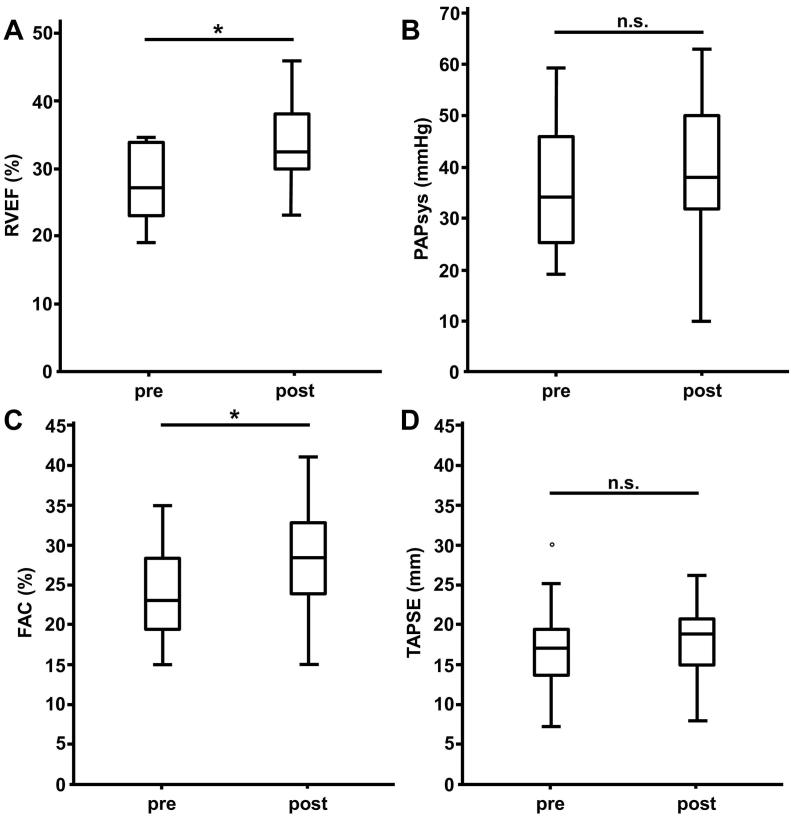
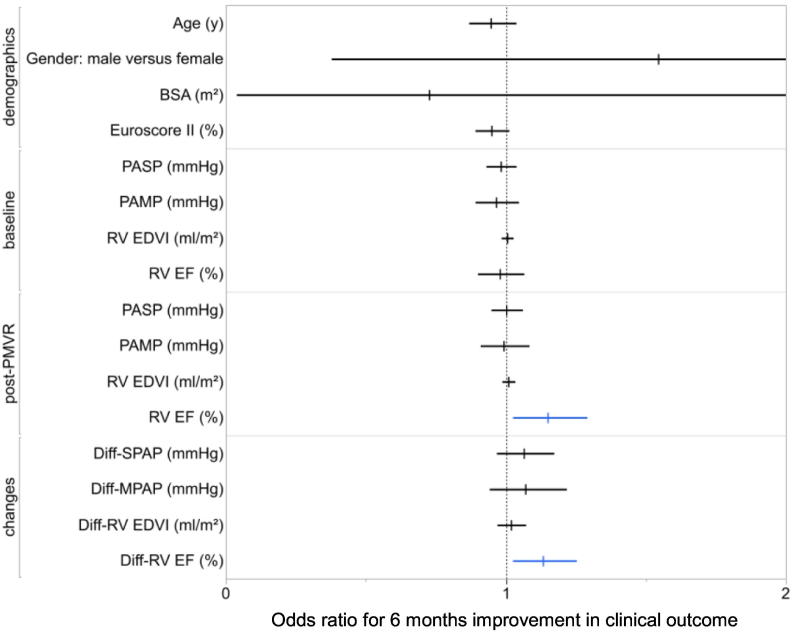
Results: In the overall collective, the 3D RV-EF before and after PMVR showed no significant change (p = 0.16). While there was a significant increase of the fractional area change (FAC, from 23 [19-29] % to 28 [24-33] %, p = 0.001), no significant change of the tricuspid annular plane systolic excursion (TAPSE, from 17 ± 6 mm to 18 ± 5 mm (standard deviation), p = 0.33) was observed. Regarding patients with a reduced RV-EF (< 35%), a significant RV-EF improvement was observed (from 27 [23-34] % to 32.5 [30-39] % (p = 0.001). 71.4% of patients had an improved clinical outcome (improvement in 6-minute walk test and/or improvement in NYHA class of more than one grade), whereas clinical outcome did not improve in 28.6% of patients. Using univariate logistic regression analysis, the post-PMVR RV-EF (OR 1.15: 95% CI 1.02-1.29; p = 0.02) and the change in RV-EF (OR 1.13: 95% CI 1.02-1.25; p = 0.02) were significant predictors for improved clinical outcome at 6 months follow up.
Conclusion: Thus, RV function may be an important non-invasive parameter to add to the predictive parameters indicating a potential clinical benefit from treatment of severe mitral regurgitation using PMVR.
Keywords: 3D-echocardiography; 3DE, 3D-echocardiography; ACE, angiotensin converting enzyme; DMR, degenerative mitral regurgitation; EDV, end-diastolic volume; EF, ejection fraction; ESV, end-systolic volume; Echocardiography; FAC, fractional area change; FMR, functional mitral regurgitation; LA, left atrium; LV, left ventricle; LVOT, left ventricular outflow tract; MR, mitral regurgitation; MRI, magnetic resonance imaging; Mitral regurgitation; NYHA, New York heart association functional classification; Outcome; PAMP, pulmonary artery mean pressure; PASP, pulmonary artery systolic pressure; PCWP, pulmonary capillary wedge pressure; PMVR, percutaneous mitral valve repair; Percutaneous mitral valve repair; RV function; RV, right ventricle; TAPSE, tricuspid annular plane systolic excursion; TAVR, transcatheter aortic valve replacement; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography.
Conflict of interest statement
Dr. H. F. Langer and Dr. P. Seizer were reimbursed for PMVR training courses by Abbott Vascular, otherwise we have no potential conflict of interest to declare.
Figures
Similar articles
-
Improved mid-term stability of MR reduction with an increased number of clips after percutaneous mitral valve repair in functional MR.Int J Cardiol Heart Vasc. 2023 Mar 10;45:101190. doi: 10.1016/j.ijcha.2023.101190. eCollection 2023 Apr. Int J Cardiol Heart Vasc. 2023. PMID: 36941997 Free PMC article.
-
Novel Right Ventricular Function Parameters can Identify Short-Term Nonresponders to Transcatheter Edge-to-Edge Repair for Mitral Regurgitation.Am J Cardiol. 2025 Jul 15;247:13-20. doi: 10.1016/j.amjcard.2025.03.034. Epub 2025 Apr 1. Am J Cardiol. 2025. PMID: 40174700
-
Impact of percutaneous mitral valve repair using the MitraClip system on tricuspid regurgitation.EuroIntervention. 2016 Apr 8;11(14):e1680-6. doi: 10.4244/EIJV11I14A320. EuroIntervention. 2016. PMID: 27056128
-
Percutaneous Edge-to-Edge Mitral Valve Repair: Beyond the Left Heart.J Am Soc Echocardiogr. 2021 Oct;34(10):1038-1045. doi: 10.1016/j.echo.2021.05.013. Epub 2021 May 27. J Am Soc Echocardiogr. 2021. PMID: 34052316 Review.
-
Right Ventricular and Outflow Tract Functional Characteristics After Repair of Tetralogy of Fallot with Major Aortopulmonary Collaterals.Pediatr Cardiol. 2024 Apr;45(4):795-803. doi: 10.1007/s00246-024-03412-0. Epub 2024 Feb 16. Pediatr Cardiol. 2024. PMID: 38360921 Review.
Cited by
-
Three-Dimensional Echocardiography Assessment of Right Ventricular Volumes and Function: Technological Perspective and Clinical Application.Diagnostics (Basel). 2022 Mar 25;12(4):806. doi: 10.3390/diagnostics12040806. Diagnostics (Basel). 2022. PMID: 35453854 Free PMC article. Review.
-
Acute changes of global and longitudinal right ventricular function: an exploratory analysis in patients undergoing open-chest mitral valve surgery, percutaneous mitral valve repair and off-pump coronary artery bypass grafting.Cardiovasc Ultrasound. 2020 Aug 12;18(1):32. doi: 10.1186/s12947-020-00218-x. Cardiovasc Ultrasound. 2020. PMID: 32787878 Free PMC article.
-
Right Ventricular Function Improves Early After Percutaneous Mitral Valve Repair in Patients Suffering From Severe Mitral Regurgitation.Front Cardiovasc Med. 2022 Mar 17;9:830944. doi: 10.3389/fcvm.2022.830944. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35369337 Free PMC article.
References
-
- Magunia H., Dietrich C., Langer H.F., Schibilsky D., Schlensak C., Rosenberger P., Nowak-Machen M. 3d echocardiography derived right ventricular function is associated with right ventricular failure and mid-term survival after left ventricular assist device implantation. Int. J. Cardiol. 2018;272:348–355. - PubMed
-
- Nagata Y., Wu V.C., Kado Y., Otani K., Lin F.C., Otsuji Y., Negishi K., Takeuchi M. Prognostic value of right ventricular ejection fraction assessed by transthoracic 3d echocardiography. Circ Cardiovasc Imaging. 2017;10 - PubMed
-
- Gripari P., Tamborini G., Bottari V., Maffessanti F., Carminati M.C., Muratori M., Vignati C., Bartorelli A.L., Alamanni F., Pepi M. Three-dimensional transthoracic echocardiography in the comprehensive evaluation of right and left heart chamber remodeling following percutaneous mitral valve repair. Journal of the American Society of Echocardiography: Official Publication of the American Society of Echocardiography. 2016;29:946–954. - PubMed
-
- Zanobini M., Loardi C., Poggio P., Tamborini G., Veglia F., Di Minno A., Myasoedova V., Mammana L.F., Biondi R., Pepi M., Alamanni F., Saccocci M. The impact of pericardial approach and myocardial protection onto postoperative right ventricle function reduction. J. Cardiothorac. Surg. 2018;13:55. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
