

Population Pharmacokinetic Analysis for Imipenem-Relebactam in Healthy Volunteers and Patients With Bacterial Infections
- PMID: 31508899
- PMCID: PMC6813166
- DOI: 10.1002/psp4.12462
Population Pharmacokinetic Analysis for Imipenem-Relebactam in Healthy Volunteers and Patients With Bacterial Infections
Abstract
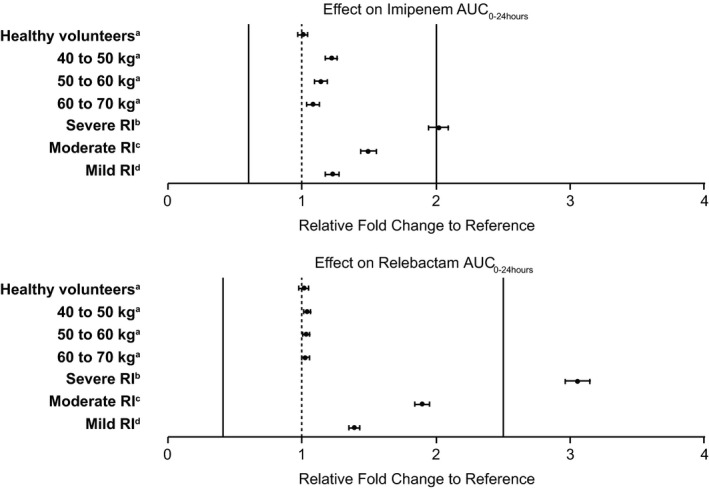
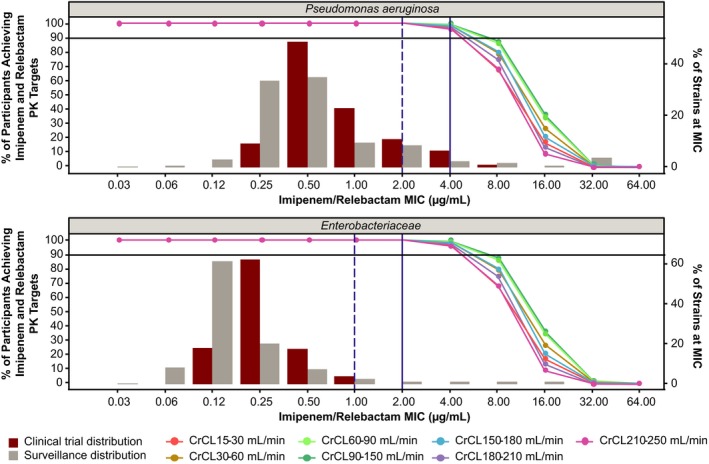
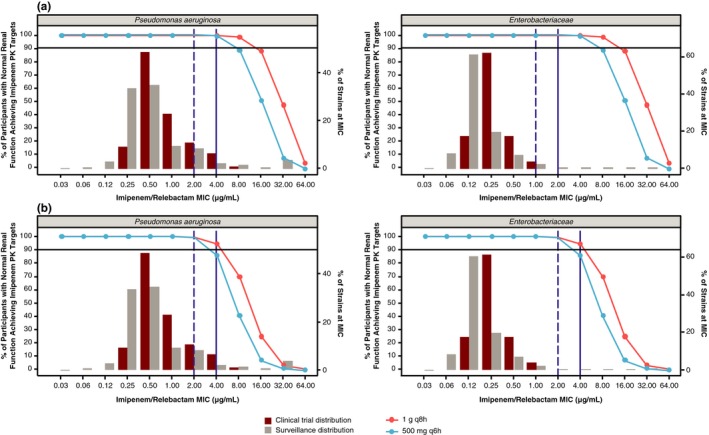
Relebactam is a small-molecule β-lactamase inhibitor developed as a fixed-dose combination with imipenem/cilastatin. The pharmacokinetics of relebactam and imipenem across 10 clinical studies were analyzed using data from adult healthy volunteers and patients with bacterial infections. Renal function estimated by creatinine clearance significantly affected the clearance of both compounds, whereas weight and health status were of less clinical significance. Simulations were used to calculate probability of joint target attainment (ratio of free drug area under the curve from 0 to 24 hours to minimum inhibitory concentration (MIC) for relebactam and percentage of time the free drug concentration exceeded the MIC for imipenem) for the proposed imipenem/relebactam dose of 500/250 mg, with adjustments for patients with renal impairment, administered as a 30-minute intravenous infusion four times daily. These dosing regimens provide sufficient antibacterial coverage (MIC ≤ 4 μg/mL) for all renal groups.
© 2019 Merck Sharp & Dohme Corp. a subsidiary of Merck & Co. Inc. CPT: Pharmacometrics & Systems Pharmacology published by Wiley Periodicals, Inc. on behalf of the American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
M.L., M.X., K.Y., and M.L.R. are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA. P.B. was a former employee of MSD at the time of study conduct and initial drafting of the manuscript. P.P., K.W., W.C., and P.K. are employees of Certara USA, Inc. or its subsidiaries, which provides consulting services to Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA.
Figures
Similar articles
-
A translational pharmacokinetic/pharmacodynamic model to characterize bacterial kill in the presence of imipenem-relebactam.Int J Infect Dis. 2019 Dec;89:55-61. doi: 10.1016/j.ijid.2019.08.026. Epub 2019 Aug 31. Int J Infect Dis. 2019. PMID: 31479762
-
Pharmacokinetics, Safety, and Tolerability of Imipenem/Cilastatin/Relebactam in Children with Confirmed or Suspected Gram-Negative Bacterial Infections: A Phase 1b, Open-Label, Single-Dose Clinical Trial.J Clin Pharmacol. 2023 Dec;63(12):1387-1397. doi: 10.1002/jcph.2334. Epub 2023 Sep 2. J Clin Pharmacol. 2023. PMID: 37562063 Clinical Trial.
-
Imipenem/relebactam pharmacokinetics in critically ill patients supported on extracorporeal membrane oxygenation.J Antimicrob Chemother. 2024 May 2;79(5):1118-1125. doi: 10.1093/jac/dkae079. J Antimicrob Chemother. 2024. PMID: 38517465
-
Imipenem-Relebactam and Meropenem-Vaborbactam: Two Novel Carbapenem-β-Lactamase Inhibitor Combinations.Drugs. 2018 Jan;78(1):65-98. doi: 10.1007/s40265-017-0851-9. Drugs. 2018. PMID: 29230684 Review.
-
Imipenem-Cilastatin-Relebactam: A Novel β-Lactam-β-Lactamase Inhibitor Combination for the Treatment of Multidrug-Resistant Gram-Negative Infections.Pharmacotherapy. 2020 Apr;40(4):343-356. doi: 10.1002/phar.2378. Epub 2020 Mar 9. Pharmacotherapy. 2020. PMID: 32060929 Review.
Cited by
-
Microbiological, Clinical, and PK/PD Features of the New Anti-Gram-Negative Antibiotics: β-Lactam/β-Lactamase Inhibitors in Combination and Cefiderocol-An All-Inclusive Guide for Clinicians.Pharmaceuticals (Basel). 2022 Apr 12;15(4):463. doi: 10.3390/ph15040463. Pharmaceuticals (Basel). 2022. PMID: 35455461 Free PMC article. Review.
-
Rationale and evidence for the use of new beta-lactam/beta-lactamase inhibitor combinations and cefiderocol in critically ill patients.Ann Intensive Care. 2023 Jul 18;13(1):65. doi: 10.1186/s13613-023-01153-6. Ann Intensive Care. 2023. PMID: 37462830 Free PMC article. Review.
-
Therapeutic drug monitoring (TDM) of β-lactam/β-lactamase inhibitor (BL/BLI) drug combinations: insights from a pharmacometric simulation study.J Antimicrob Chemother. 2025 Jan 3;80(1):79-86. doi: 10.1093/jac/dkae375. J Antimicrob Chemother. 2025. PMID: 39436757 Free PMC article.
-
Durlobactam to boost the clinical utility of standard of care β-lactams against Mycobacterium abscessus lung disease.Antimicrob Agents Chemother. 2025 Jan 31;69(1):e0104624. doi: 10.1128/aac.01046-24. Epub 2024 Nov 20. Antimicrob Agents Chemother. 2025. PMID: 39565116 Free PMC article.
-
Mutant prevention concentrations, in vitro resistance evolution dynamics, and mechanisms of resistance to imipenem and imipenem/relebactam in carbapenem-susceptible Klebsiella pneumoniae isolates showing ceftazidime/avibactam resistance.Antimicrob Agents Chemother. 2024 Dec 5;68(12):e0112024. doi: 10.1128/aac.01120-24. Epub 2024 Nov 15. Antimicrob Agents Chemother. 2024. PMID: 39545736 Free PMC article.
References
-
- Blizzard, T.A. et al Discovery of MK‐7655, a beta‐lactamase inhibitor for combination with Primaxin® . Bioorg. Med. Chem. Lett. 24, 780–785 (2014). - PubMed
-
- PRIMAXIN® (imipenem and cilastatin) [prescribing information] . (Merck Sharp & Dohme Corp., a subsidiary of Merck & Co. Inc.,Whitehouse Station, NJ, 2018).
-
- Livermore, D.M. , Warner, M. & Mushtaq, S. Activity of MK‐7655 combined with imipenem against Enterobacteriaceae and Pseudomonas aeruginosa. J. Antimicrob. Chemother. 68, 2286–2290 (2013). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
