

Dual-Energy Computed Tomography Detection of Cardiovascular Monosodium Urate Deposits in Patients With Gout
- PMID: 31509156
- PMCID: PMC6739730
- DOI: 10.1001/jamacardio.2019.3201
Dual-Energy Computed Tomography Detection of Cardiovascular Monosodium Urate Deposits in Patients With Gout
Abstract
Importance: The prevalence of gout has increased in recent decades. Several clinical studies have demonstrated an association between gout and coronary heart disease, but direct cardiovascular imaging of monosodium urate (MSU) deposits by using dual-energy computed tomography (DECT) has not been reported to date.
Objective: To compare coronary calcium score and cardiovascular MSU deposits detected by DECT in patients with gout and controls.
Design, setting, and participants: This prospective Health Insurance Portability and Accountability Act-compliant study included patients with gout and controls who presented to a rheumatologic clinic from January 1, 2017, to November 1, 2018. All consecutive patients underwent DECT to assess coronary calcium score and MSU deposits in aorta and coronary arteries. In addition, cadavers were assessed by DECT for cardiovascular MSU deposits and verified by polarizing microscope. Analysis began in January 2017.
Main outcomes and measures: Detection rate of cardiovascular MSU deposits using DECT in patients with gout and control group patients without a previous history of gout or inflammatory rheumatic diseases.
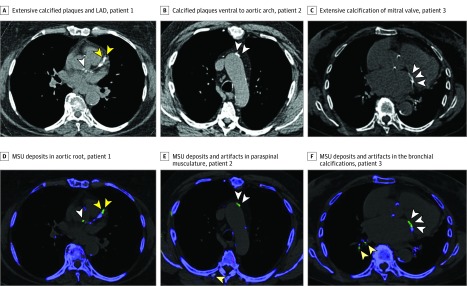
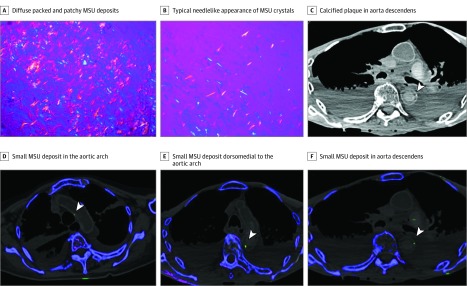
Results: A total of 59 patients with gout (mean [SD] age, 59 [5.7] years; range, 47-89 years), 47 controls (mean [SD] age, 70 [10.4] years; range, 44-86 years), and 6 cadavers (mean [SD] age at death, 76 [17] years; range, 56-95 years) were analyzed. The frequency of cardiovascular MSU deposits was higher among patients with gout (51 [86.4%]) compared with controls (7 [14.9%]) (χ2 = 17.68, P < .001), as well as coronary MSU deposits among patients with gout (19 [32.2%]) vs controls (2 [4.3%]) (χ2 = 8.97, P = .003). Coronary calcium score was significantly higher among patients with gout (900 Agatston units [AU]; 95% CI, 589-1211) compared with controls (263 AU; 95% CI, 76-451; P = .001) and also significantly higher among 58 individuals with cardiovascular MSU deposits (950 AU; 95% CI, 639-1261) compared with 48 individuals without MSU deposits (217 AU; 95% CI, 37-397; P < .001). Among 6 cadavers, 3 showed cardiovascular MSU deposits, which were verified by polarizing light microscope.
Conclusion and relevance: Dual-energy computed tomography demonstrates cardiovascular MSU deposits, as confirmed by polarized light microscopy. Cardiovascular MSU deposits were detected by DECT significantly more often in patients with gout compared with controls and were associated with higher coronary calcium score. This new modality may be of importance in gout population being at risk from cardiovascular disease.
Conflict of interest statement
Figures

Comment in
-
Identification of Cardiovascular Monosodium Urate Crystal Deposition in Patients With Gout Using Dual-Energy Computed Tomography-Reply.JAMA Cardiol. 2020 Apr 1;5(4):486-487. doi: 10.1001/jamacardio.2019.5807. JAMA Cardiol. 2020. PMID: 32022824 No abstract available.
-
Identification of Cardiovascular Monosodium Urate Crystal Deposition in Patients With Gout Using Dual-Energy Computed Tomography.JAMA Cardiol. 2020 Apr 1;5(4):486. doi: 10.1001/jamacardio.2019.5804. JAMA Cardiol. 2020. PMID: 32022840 No abstract available.
Similar articles
-
Association between coronary monosodium urate deposits at DECT and high-risk coronary plaque phenotypes and other features in gout patients.Eur Radiol Exp. 2025 Aug 11;9(1):73. doi: 10.1186/s41747-025-00611-z. Eur Radiol Exp. 2025. PMID: 40790104 Free PMC article.
-
Monosodium Urate Crystal Deposition in Coronary Artery Plaque by 128-Slice Dual-Energy Computed Tomography: An Ex Vivo Phantom and In Vivo Study.J Comput Assist Tomogr. 2021 Nov-Dec 01;45(6):856-862. doi: 10.1097/RCT.0000000000001222. J Comput Assist Tomogr. 2021. PMID: 34469909
-
Prevalence of Monosodium Urate (MSU) Deposits in Cadavers Detected by Dual-Energy Computed Tomography (DECT).Diagnostics (Basel). 2022 May 16;12(5):1240. doi: 10.3390/diagnostics12051240. Diagnostics (Basel). 2022. PMID: 35626395 Free PMC article.
-
What Has Dual Energy CT Taught Us About Gout?Curr Rheumatol Rep. 2021 Jul 14;23(9):71. doi: 10.1007/s11926-021-01035-5. Curr Rheumatol Rep. 2021. PMID: 34259946 Review.
-
Review: The Role of Dual-Energy Computed Tomography in Detecting Monosodium Urate Deposits in Vascular Tissues.Curr Rheumatol Rep. 2024 Aug;26(8):302-310. doi: 10.1007/s11926-024-01151-y. Epub 2024 May 13. Curr Rheumatol Rep. 2024. PMID: 38739298 Free PMC article. Review.
Cited by
-
A comparative study of postadrenalectomy hyperuricemia and renal impairment in patients with unilateral primary aldosteronism: does histopathology subtype matter?BMC Nephrol. 2024 Oct 13;25(1):347. doi: 10.1186/s12882-024-03750-4. BMC Nephrol. 2024. PMID: 39396977 Free PMC article.
-
Utility of Ultrasound and Dual Energy CT in Crystal Disease Diagnosis and Management.Curr Rheumatol Rep. 2020 Apr 15;22(5):15. doi: 10.1007/s11926-020-0890-1. Curr Rheumatol Rep. 2020. PMID: 32291581 Review.
-
Gout: global epidemiology, risk factors, comorbidities and complications: a narrative review.BMC Musculoskelet Disord. 2024 Dec 19;25(1):1047. doi: 10.1186/s12891-024-08180-9. BMC Musculoskelet Disord. 2024. PMID: 39702222 Free PMC article. Review.
-
Detection of monosodium urate depositions and atherosclerotic plaques in the cardiovascular system by dual-energy computed tomography.Heliyon. 2024 Jan 17;10(2):e24548. doi: 10.1016/j.heliyon.2024.e24548. eCollection 2024 Jan 30. Heliyon. 2024. PMID: 38304777 Free PMC article.
-
A nonlinear correlation between the serum uric acid to creatinine ratio and the prevalence of hypertension: a large cross-sectional population-based study.Ren Fail. 2024 Dec;46(1):2296002. doi: 10.1080/0886022X.2023.2296002. Epub 2024 Jan 8. Ren Fail. 2024. PMID: 38186345 Free PMC article.
