

The Risk for Glucose Intolerance after Gestational Diabetes Mellitus since the Introduction of the IADPSG Criteria: A Systematic Review and Meta-Analysis
- PMID: 31510081
- PMCID: PMC6780861
- DOI: 10.3390/jcm8091431
The Risk for Glucose Intolerance after Gestational Diabetes Mellitus since the Introduction of the IADPSG Criteria: A Systematic Review and Meta-Analysis
Abstract
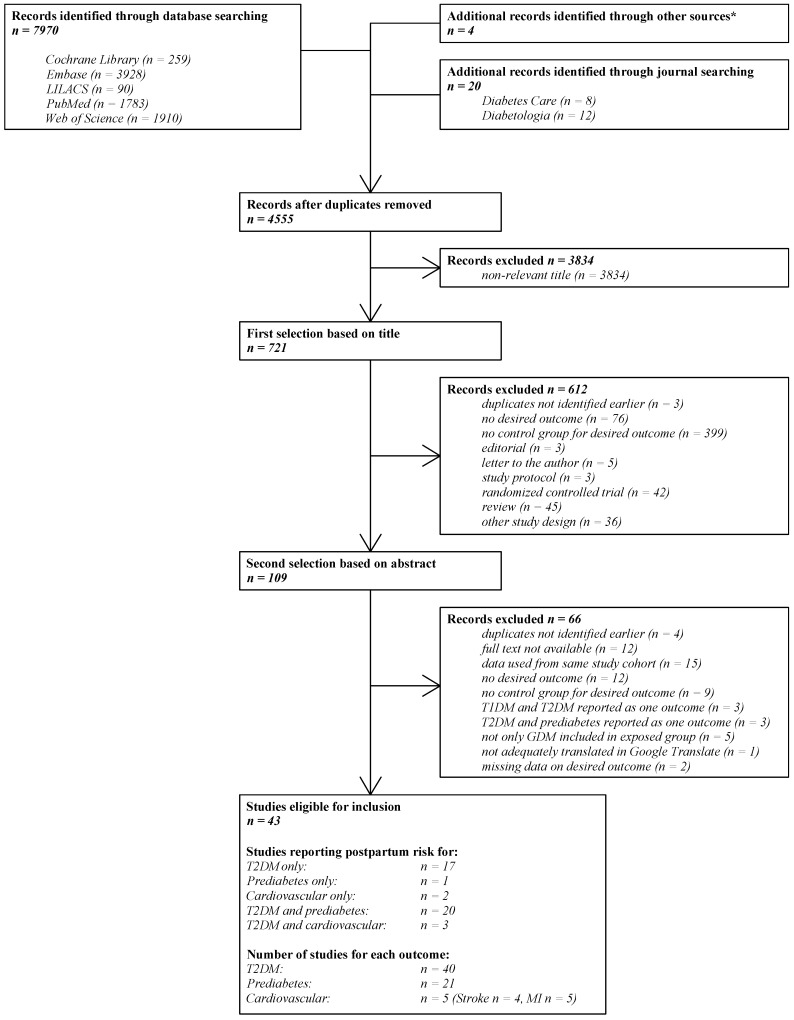
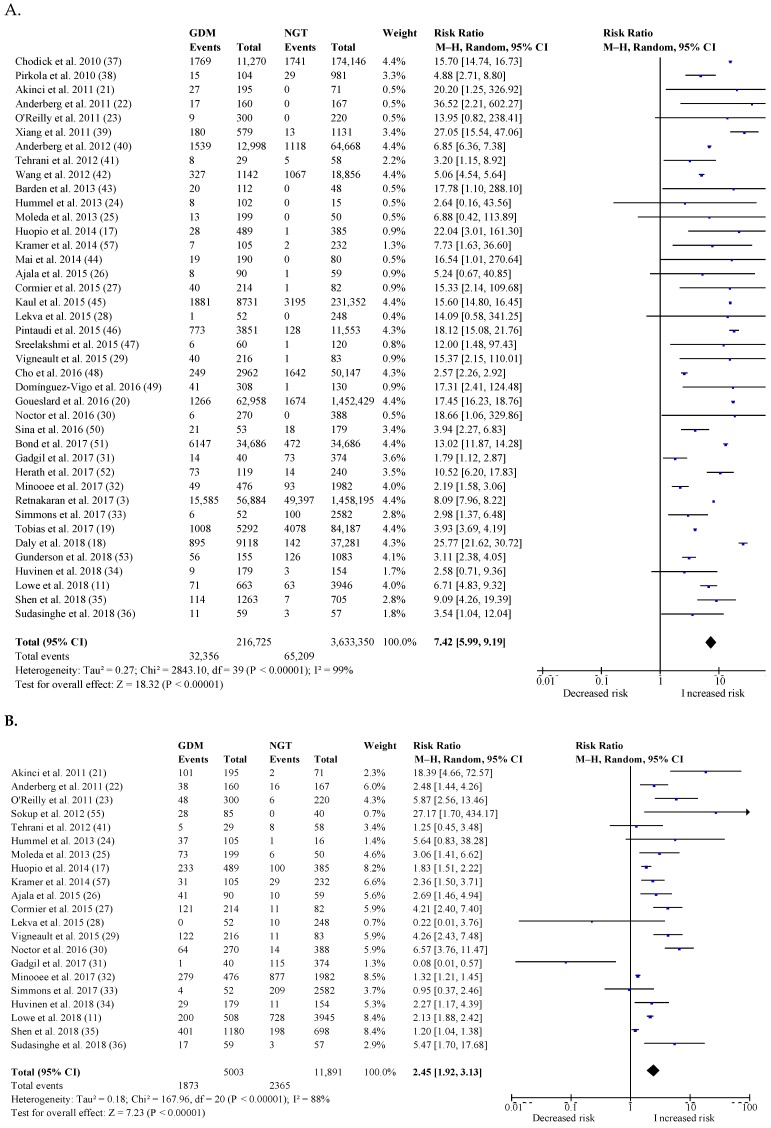
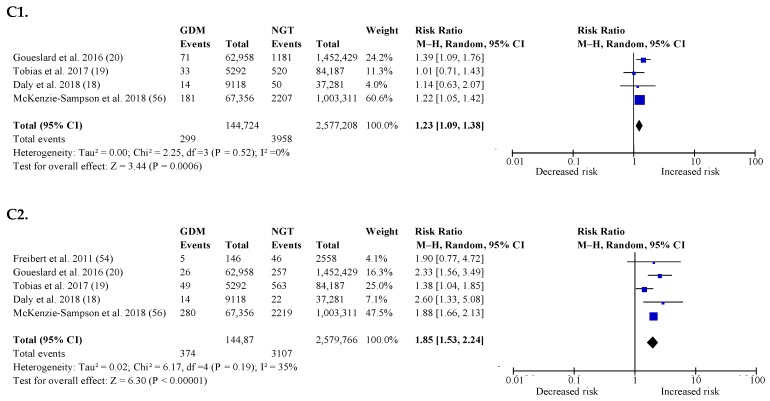
The aim of the study was to assess the postpartum risk for glucose intolerance since the introduction of the 'International Association of Diabetes and Pregnancy Study Groups' (IADPSG) criteria for gestational diabetes mellitus (GDM). Studies published since 2010 were included, which evaluated the risk for type 2 diabetes mellitus (T2DM), impaired glucose tolerance (IGT), and cardiovascular (CV) events in women with previous GDM compared to normal glucose tolerant women. We included forty-three studies, evaluating 4,923,571 pregnant women of which 5.8% (284,312) had a history of GDM. Five studies used IADPSG criteria (n = 6174 women, 1314 with GDM). The overall pooled relative risk (RR) for postpartum T2DM was 7.42 (95% CI: 5.99-9.19) and the RR for postpartum T2DM with IADPSG criteria was 6.45 (95% CI: 4.74-8.77) compared to the RR of 9.08 (95% CI: 6.96-11.85; p = 0.17) for postpartum T2DM based on other diagnostic criteria. The RR for postpartum IGT was 2.45 (95% CI: 1.92-3.13), independent of the criteria used. None of the available studies with IADPSG criteria evaluated the risk for CV events. Women with a history of GDM based on the IADPSG criteria have a similarly increased risk for postpartum glucose intolerance compared to GDM based on other diagnostic criteria. More studies with GDM based on the IADPSG criteria are needed to increase the quality of evidence concerning the long-term metabolic risk.
Keywords: International Association of Diabetes and Pregnancy Study Groups (IADPSG); diagnostic criteria; gestational diabetes mellitus; glucose intolerance; impaired glucose tolerance; myocardial infarction; postpartum; stroke; type 2 diabetes.
Conflict of interest statement
The authors declare that there is no conflict of interest associated with this manuscript.
Figures
References
-
- Metzger B.E., Buchanan T.A., Coustan D.R., de Leiva A., Dunger D.B., Hadden D.R., Hod M., Kitzmiller J.L., Kjos S.L., Oats J.N., et al. Summary and recommendations of the Fifth International Workshop-Conference on Gestational Diabetes Mellitus. Diabetes Care. 2007;30(Suppl. 2):S251–S260. doi: 10.2337/dc07-s225. - DOI - PubMed
-
- HAPO Study Cooperative Research Group. Metzger B.E., Lowe L.P., Dyer A.R., Trimble E.R., Chaovarindr U., Coustan D.R., Hadden D.R., McCance D.R., Hod M., et al. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008;358:1991–2002. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
