

Transfusion practice in the non-bleeding critically ill: an international online survey-the TRACE survey
- PMID: 31511083
- PMCID: PMC6737617
- DOI: 10.1186/s13054-019-2591-6
Transfusion practice in the non-bleeding critically ill: an international online survey-the TRACE survey
Abstract
Background: Over the last decade, multiple large randomized controlled trials have studied alternative transfusion strategies in critically ill patients, demonstrating the safety of restrictive transfusion strategies. Due to the lack of international guidelines specific for the intensive care unit (ICU), we hypothesized that a large heterogeneity in transfusion practice in this patient population exists. The aims of this study were to describe the current transfusion practices and identify the knowledge gaps.
Methods: An online, anonymous, worldwide survey among ICU physicians was performed evaluating red blood cell, platelet and plasma transfusion practices. Furthermore, the presence of a hospital- or ICU-specific transfusion guideline was asked. Only completed surveys were analysed.
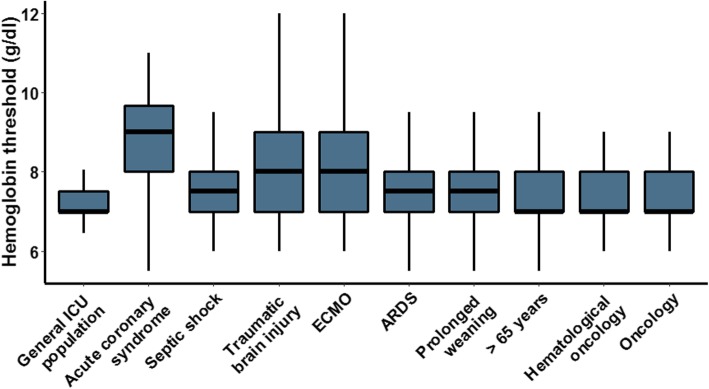
Results: Nine hundred forty-seven respondents filled in the survey of which 725 could be analysed. Hospital transfusion protocol available in their ICU was reported by 53% of the respondents. Only 29% of respondents used an ICU-specific transfusion guideline. The reported haemoglobin (Hb) threshold for the general ICU population was 7 g/dL (7-7). The highest reported variation in transfusion threshold was in patients on extracorporeal membrane oxygenation or with brain injury (8 g/dL (7.0-9.0)). Platelets were transfused at a median count of 20 × 109 cells/L IQR (10-25) in asymptomatic patients, but at a higher count prior to invasive procedures (p < 0.001). In patients with an international normalized ratio (INR) > 3, 43% and 57% of the respondents would consider plasma transfusion without any upcoming procedures or prior to a planned invasive procedure, respectively. Finally, doctors with base specialty in anaesthesiology transfused critically ill patients more liberally compared to internal medicine physicians.
Conclusion: Red blood cell transfusion practice for the general ICU population is restrictive, while for different subpopulations, higher Hb thresholds are applied. Furthermore, practice in plasma and platelet transfusion is heterogeneous, and local transfusion guidelines are lacking in the majority of the ICUs.
Keywords: Critically ill; Plasma; Platelets; Red blood cells; Transfusion practice.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Walsh TS, Stanworth SJ, Prescott RJ, Lee RJ, Watson DM, Wyncoll D, et al. Prevalence, management, and outcomes of critically ill patients with prothrombin time prolongation in United Kingdom intensive care units. Crit Care Med. 2010;38(10):1939–1946. doi: 10.1097/CCM.0b013e3181eb9d2b. - DOI - PubMed
-
- Whitaker BI, Rajbhandary S, Harris A. 2013 AABB Blood Survey Report. 2013 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
