

Plasma Galactose-Deficient IgA1 and C3 and CKD Progression in IgA Nephropathy
- PMID: 31511226
- PMCID: PMC6777583
- DOI: 10.2215/CJN.13711118
Plasma Galactose-Deficient IgA1 and C3 and CKD Progression in IgA Nephropathy
Abstract
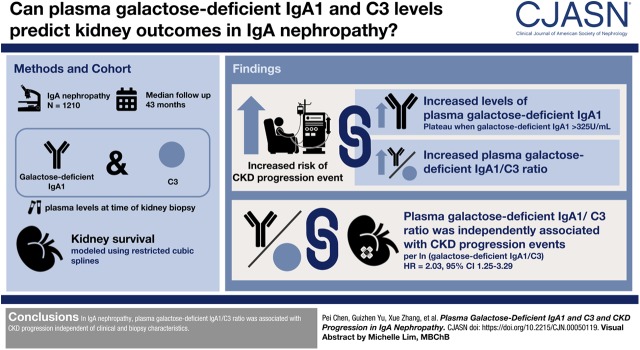
Background and objectives: Increased circulating galactose-deficient IgA1 and subsequently complement activation both play important roles in the pathophysiology of IgA nephropathy. However, their relationship to disease severity and progression remains unclear.
Design, setting, participants, & measurements: We assessed 1210 participants in a cohort study of biopsy-proven IgA nephropathy at Peking University First Hospital. Plasma concentrations of galactose-deficient IgA1 and complement component C3 were measured at the time of biopsy. We tested associations of galactose-deficient IgA1 and galactose-deficient IgA1/C3 ratio with CKD progression event, defined as ESKD or 50% decline in eGFR, using Cox proportional hazards models and restricted cubic splines.
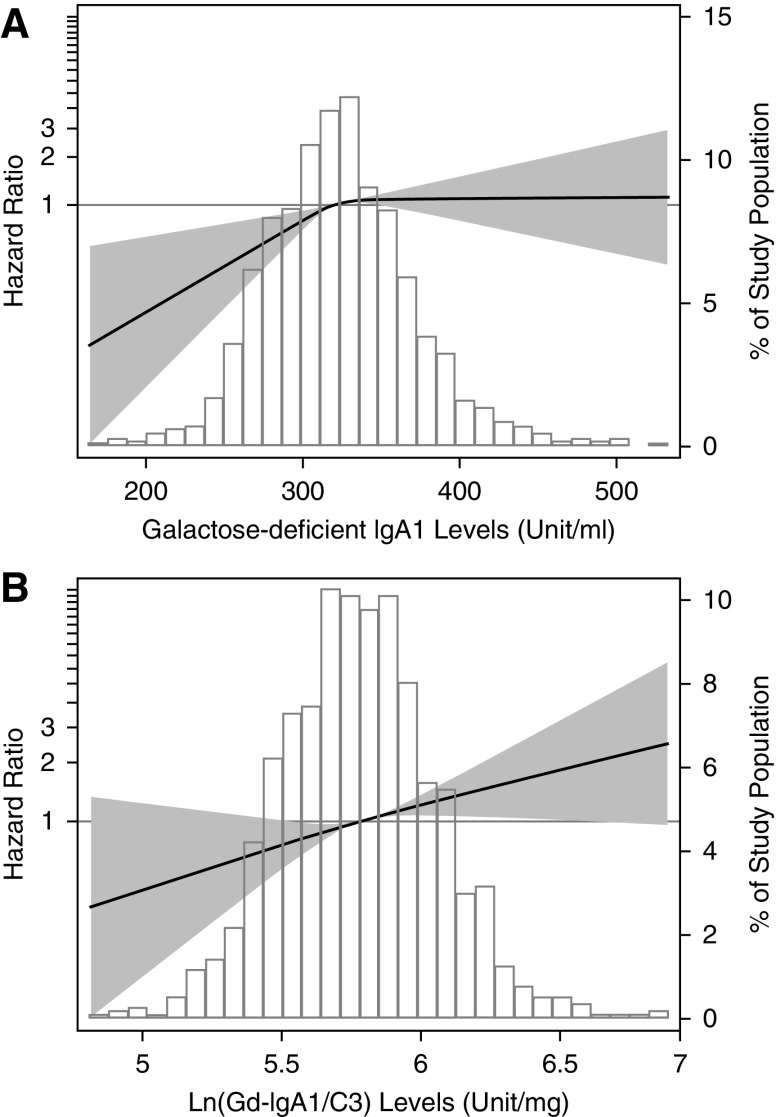
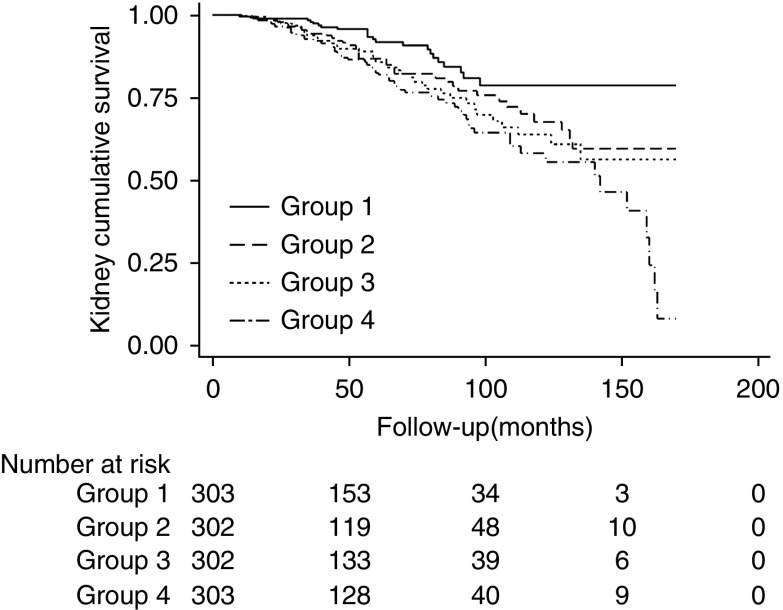
Results: After a median follow-up of 43 months (interquartile range, 24-76 months), 172 (14%) participants reached the CKD progression event. The association of galactose-deficient IgA1 levels and CKD progression event showed a nonlinear relationship. The risk of CKD progression events was greater with higher plasma galactose-deficient IgA1 levels but reached a plateau when galactose-deficient IgA1>325 U/ml, whereas the risk of CKD progression events monotonically increased with higher galactose-deficient IgA1/C3 ratio. After adjustment for traditional risk factors (demographics, eGFR, proteinuria, hypertension, Oxford pathologic score, and corticosteroids/immunosuppressive therapy), higher levels of galactose-deficient IgA1/C3 ratio were independently associated with CKD progression event (per natural log-transformed [galactose-deficient IgA1/C3], hazard ratio, 2.03; 95% confidence interval [95% CI], 1.25 to 3.29; P=0.004). In reference to the first quartile of the galactose-deficient IgA1/C3 ratio, hazard ratios were 1.71 (95% CI, 1.01 to 2.89) for the second quartile, 1.55 (95% CI, 0.91 to 2.63) for the third quartile, and 2.17 (95% CI, 1.33 to 3.56) for the fourth quartile.
Conclusions: In IgA nephropathy, plasma galactose-deficient IgA1/C3 ratio was associated with CKD progression event independent of clinical and biopsy characteristics.
Keywords: IGA glomerulonephritis; IgA nephropathy; adrenal cortex hormones; biopsy; chronic kidney failure; chronic renal insufficiency; complement activation; complement c3; demography; follow-up studies; galactose; glycation; hypertension; immunoglobulin A; kidney development; proportional hazards models; proteinuria; risk factors; universities.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
Biomarkers to Predict Progression in IgA Nephropathy.Clin J Am Soc Nephrol. 2019 Oct 7;14(10):1421-1423. doi: 10.2215/CJN.09100819. Epub 2019 Sep 11. Clin J Am Soc Nephrol. 2019. PMID: 31591255 Free PMC article. No abstract available.
References
-
- D’Amico G: The commonest glomerulonephritis in the world: IgA nephropathy. Q J Med 64: 709–727, 1987 - PubMed
-
- Woo KT, Chan CM, Chin YM, Choong HL, Tan HK, Foo M, Anantharaman V, Lee GS, Chiang GS, Tan PH, Lim CH, Tan CC, Lee E, Tan HB, Fook-Chong S, Lau YK, Wong KS: Global evolutionary trend of the prevalence of primary glomerulonephritis over the past three decades. Nephron Clin Pract 116: c337–c346, 2010 - PubMed
-
- McGrogan A, Franssen CF, de Vries CS: The incidence of primary glomerulonephritis worldwide: A systematic review of the literature. Nephrol Dial Transplant 26: 414–430, 2011 - PubMed
-
- Wyatt RJ, Julian BA: IgA nephropathy. N Engl J Med 368: 2402–2414, 2013 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
