

Community-Acquired Respiratory Viruses in Transplant Patients: Diversity, Impact, Unmet Clinical Needs
- PMID: 31511250
- PMCID: PMC7399564
- DOI: 10.1128/CMR.00042-19
Community-Acquired Respiratory Viruses in Transplant Patients: Diversity, Impact, Unmet Clinical Needs
Abstract
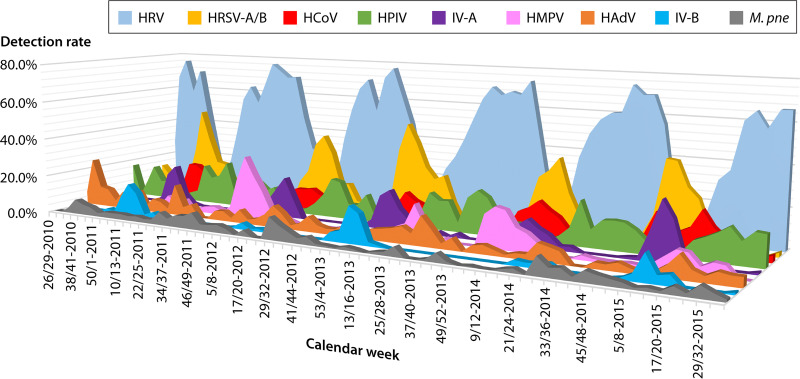
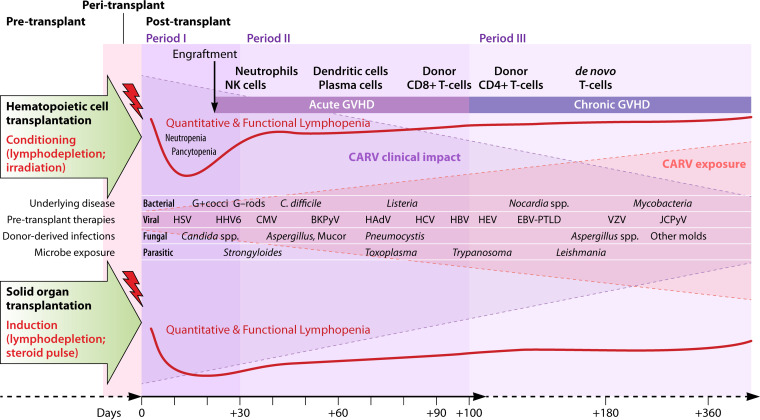
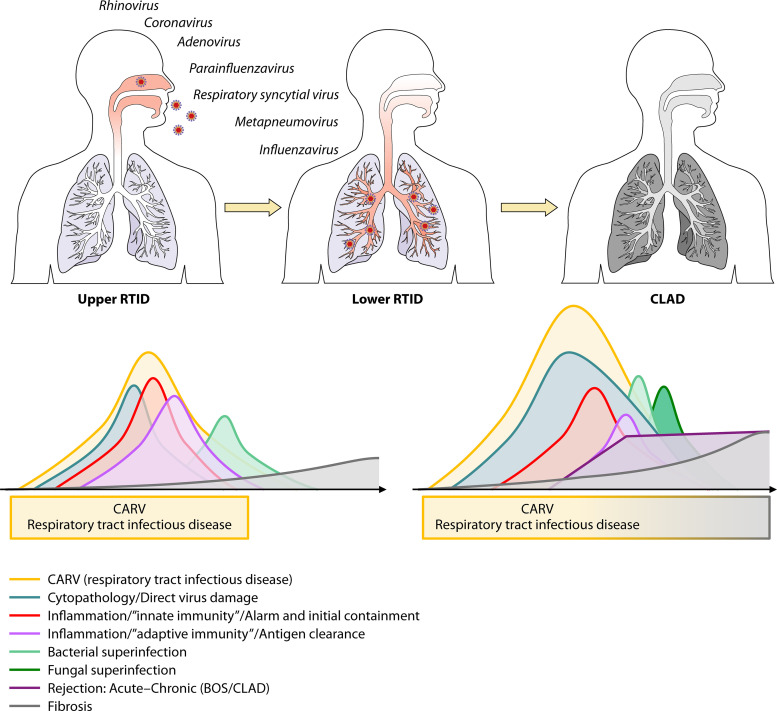
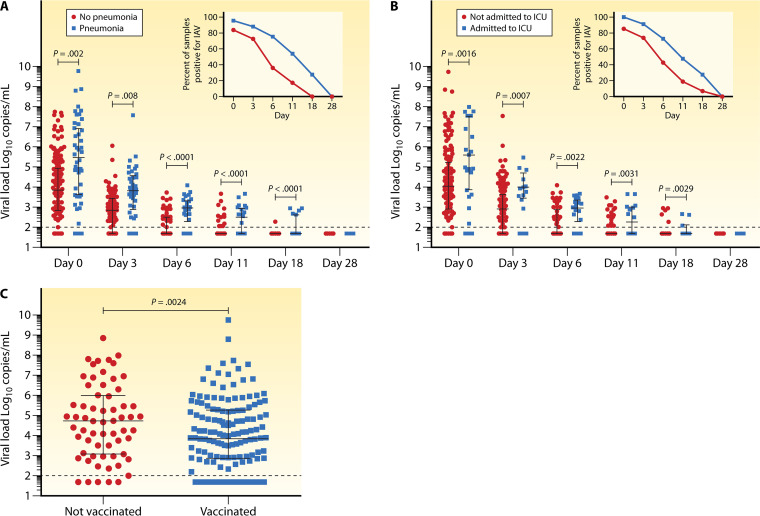
Patients undergoing solid-organ transplantation (SOT) or allogeneic hematopoietic cell transplantation (HCT) are at increased risk for infectious complications. Community-acquired respiratory viruses (CARVs) pose a particular challenge due to the frequent exposure pre-, peri-, and posttransplantation. Although influenza A and B viruses have a top priority regarding prevention and treatment, recent molecular diagnostic tests detecting an array of other CARVs in real time have dramatically expanded our knowledge about the epidemiology, diversity, and impact of CARV infections in the general population and in allogeneic HCT and SOT patients. These data have demonstrated that non-influenza CARVs independently contribute to morbidity and mortality of transplant patients. However, effective vaccination and antiviral treatment is only emerging for non-influenza CARVs, placing emphasis on infection control and supportive measures. Here, we review the current knowledge about CARVs in SOT and allogeneic HCT patients to better define the magnitude of this unmet clinical need and to discuss some of the lessons learned from human influenza virus, respiratory syncytial virus, parainfluenzavirus, rhinovirus, coronavirus, adenovirus, and bocavirus regarding diagnosis, prevention, and treatment.
Keywords: bone marrow transplantation; diagnosis; respiratory viruses; solid-organ transplantation; treatment; vaccination.
Copyright © 2019 American Society for Microbiology.
Figures
References
-
- Ison MG. 2007. Respiratory viral infections in transplant recipients. Antivir Ther 12:627–638. - PubMed
-
- Hirsch HH, Martino R, Ward KN, Boeckh M, Einsele H, Ljungman P. 2013. Fourth European Conference on Infections in Leukaemia (ECIL-4): guidelines for diagnosis and treatment of human respiratory syncytial virus, parainfluenza virus, metapneumovirus, rhinovirus, and coronavirus. Clin Infect Dis 56:258–266. doi: 10.1093/cid/cis844. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
