

Association of endothelial and glycocalyx injury biomarkers with fluid administration, development of acute kidney injury, and 90-day mortality: data from the FINNAKI observational study
- PMID: 31512003
- PMCID: PMC6738365
- DOI: 10.1186/s13613-019-0575-y
Association of endothelial and glycocalyx injury biomarkers with fluid administration, development of acute kidney injury, and 90-day mortality: data from the FINNAKI observational study
Abstract
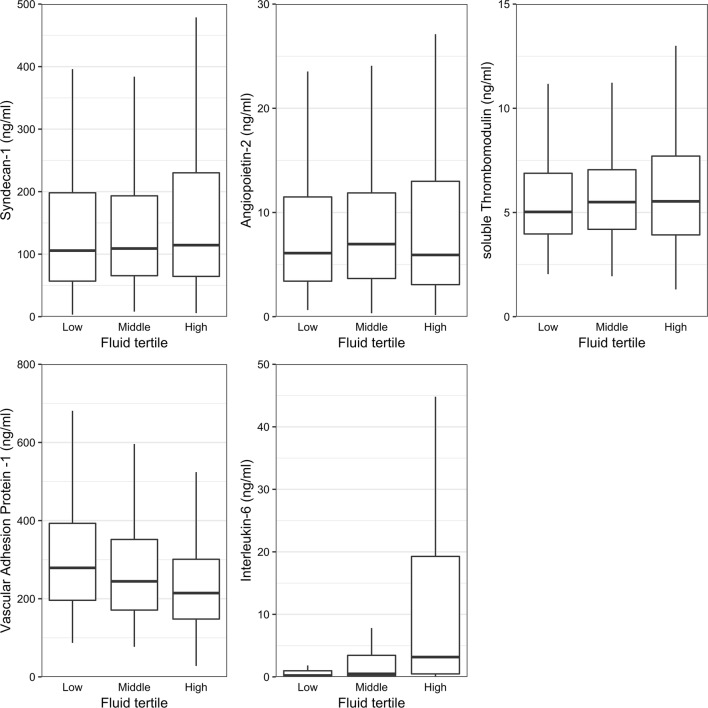
Background: Injury to endothelium and glycocalyx predisposes to vascular leak, which may subsequently lead to increased fluid requirements and worse outcomes. In this post hoc study of the prospective multicenter observational Finnish Acute Kidney Injury (FINNAKI) cohort study conducted in 17 Finnish intensive care units, we studied the association of Syndecan-1 (SDC-1), Angiopoetin-2 (Ang-2), soluble thrombomodulin (sTM), vascular adhesion protein-1 (VAP-1) and interleukin-6 (IL-6) with fluid administration and balance among septic critical care patients and their association with development of acute kidney injury (AKI) and 90-day mortality.
Results: SDC-1, Ang-2, sTM, VAP-1 and IL-6 levels were measured at ICU admission from 619 patients with sepsis. VAP-1 decreased (p < 0.001) and IL-6 increased (p < 0.001) with increasing amounts of administered fluid, but other biomarkers did not show differences according to fluid administration. In linear regression models adjusted for IL-6, only VAP-1 was significantly associated with fluid administration on day 1 (p < 0.001) and the cumulative fluid balance on day 5/ICU discharge (p = 0.001). Of 415 patients admitted without AKI, altogether 112 patients (27.0%) developed AKI > 12 h from ICU admission (AKI>12 h). They had higher sTM levels than patients without AKI, and after multivariable adjustment log, sTM level was associated with AKI>12 h with OR (95% CI) of 12.71 (2.96-54.67), p = 0.001). Ninety-day non-survivors (n = 180; 29.1%) had higher SDC-1 and sTM levels compared to survivors. After adjustment for known confounders, log SDC-1 (OR [95% CI] 2.13 [1.31-3.49], p = 0.002), log sTM (OR [95% CI] 7.35 [2.29-23.57], p < 0.001), and log Ang-2 (OR [95% CI] 2.47 [1.44-4.14], p = 0.001) associated with an increased risk for 90-day mortality. Finally, patients who had high levels of all three markers, namely, SDC-1, Ang-2 and sTM, had an adjusted OR of 5.61 (95% CI 2.67-11.79; p < 0.001) for 90-day mortality.
Conclusions: VAP-1 and IL-6 associated with fluid administration on the first ICU day. After adjusting for confounders, sTM was associated with development of AKI after 12 h from ICU admission. SDC-1, Ang-2 and sTM were independently associated with an increased risk for 90-day mortality.
Keywords: Acute kidney injury; Biomarker; Fluid balance; Fluid resuscitation; Glycocalyx; Sepsis; Soluble thrombomodulin.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
