

Progesterone and Breast Cancer
- PMID: 31512725
- PMCID: PMC7156851
- DOI: 10.1210/endrev/bnz001
Progesterone and Breast Cancer
Abstract
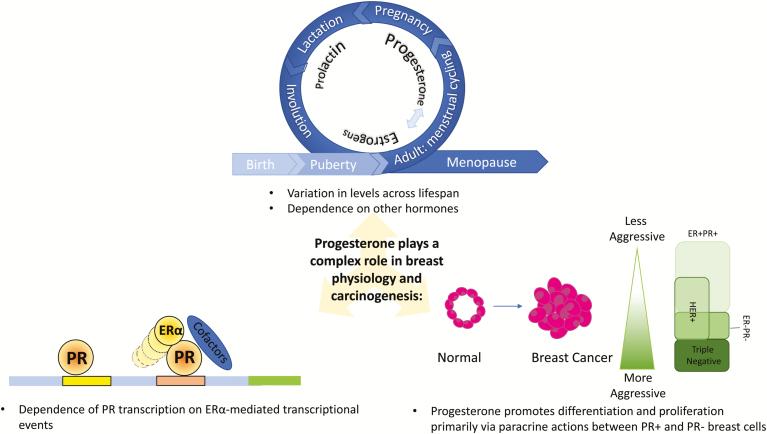
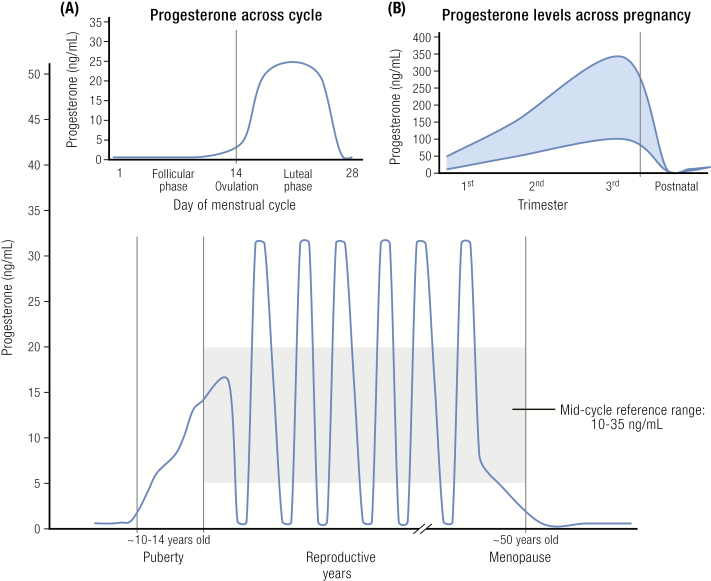
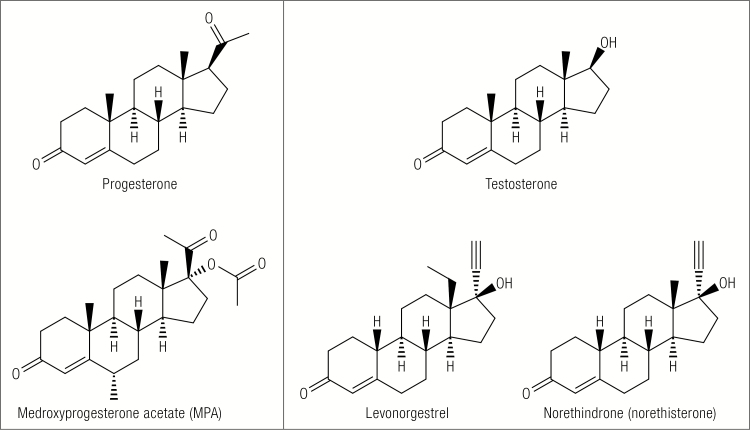
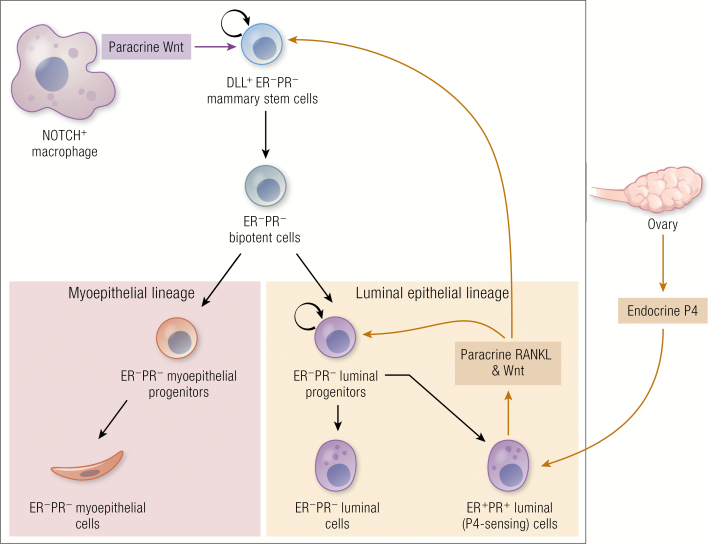
Synthetic progestogens (progestins) have been linked to increased breast cancer risk; however, the role of endogenous progesterone in breast physiology and carcinogenesis is less clearly defined. Mechanistic studies using cell culture, tissue culture, and preclinical models implicate progesterone in breast carcinogenesis. In contrast, limited epidemiologic data generally do not show an association of circulating progesterone levels with risk, and it is unclear whether this reflects methodologic limitations or a truly null relationship. Challenges related to defining the role of progesterone in breast physiology and neoplasia include: complex interactions with estrogens and other hormones (eg, androgens, prolactin, etc.), accounting for timing of blood collections for hormone measurements among cycling women, and limitations of assays to measure progesterone metabolites in blood and progesterone receptor isotypes (PRs) in tissues. Separating the individual effects of estrogens and progesterone is further complicated by the partial dependence of PR transcription on estrogen receptor (ER)α-mediated transcriptional events; indeed, interpreting the integrated interaction of the hormones may be more essential than isolating independent effects. Further, many of the actions of both estrogens and progesterone, particularly in "normal" breast tissues, are driven by paracrine mechanisms in which ligand binding to receptor-positive cells evokes secretion of factors that influence cell division of neighboring receptor-negative cells. Accordingly, blood and tissue levels may differ, and the latter are challenging to measure. Given conflicting data related to the potential role of progesterone in breast cancer etiology and interest in blocking progesterone action to prevent or treat breast cancer, we provide a review of the evidence that links progesterone to breast cancer risk and suggest future directions for filling current gaps in our knowledge.
Published by Oxford University Press on behalf of the Endocrine Society 2019.
Figures
References
-
- Zbuk K, Anand SS. Declining incidence of breast cancer after decreased use of hormone-replacement therapy: magnitude and time lags in different countries. J Epidemiol Community Health. 2012;66(1):1–7. - PubMed
-
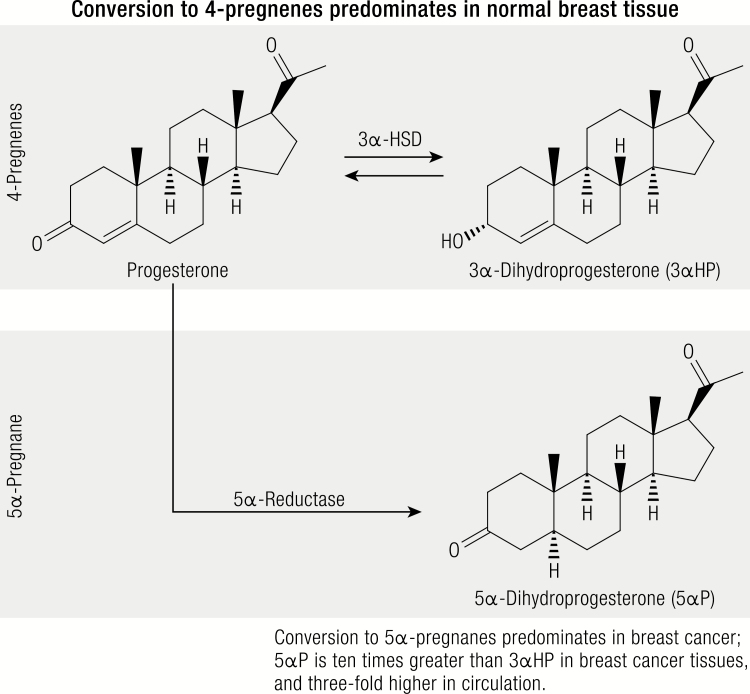
- Wiebe JP, Muzia D, Hu J, Szwajcer D, Hill SA, Seachrist JL. The 4-pregnene and 5alpha-pregnane progesterone metabolites formed in nontumorous and tumorous breast tissue have opposite effects on breast cell proliferation and adhesion. Cancer Res. 2000;60(4):936–943. - PubMed
-
- Poole AJ, Li Y, Kim Y, Lin SC, Lee WH, Lee EY. Prevention of Brca1-mediated mammary tumorigenesis in mice by a progesterone antagonist. Science. 2006;314(5804):1467–1470. - PubMed
-
- Hewitt SC, Korach KS. Progesterone action and responses in the alphaERKO mouse. Steroids. 2000;65(10–11):551–557. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
