

Informal genomic surveillance of regional distribution of Salmonella Typhi genotypes and antimicrobial resistance via returning travellers
- PMID: 31513580
- PMCID: PMC6741848
- DOI: 10.1371/journal.pntd.0007620
Informal genomic surveillance of regional distribution of Salmonella Typhi genotypes and antimicrobial resistance via returning travellers
Abstract
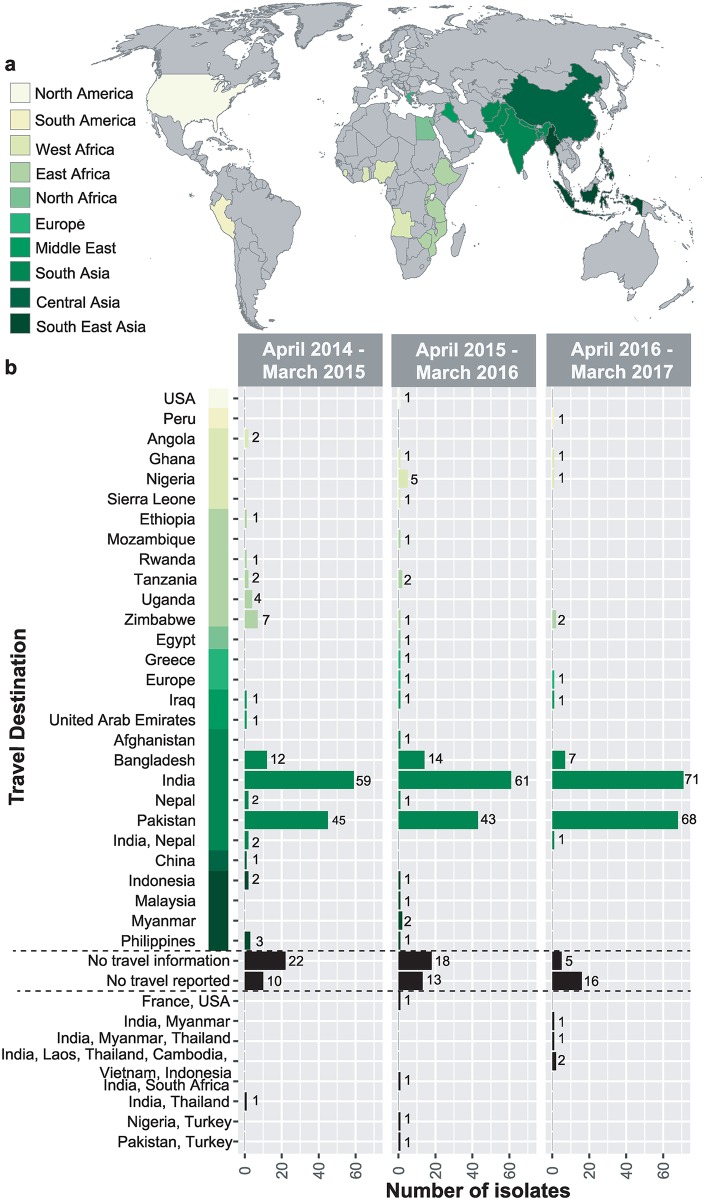
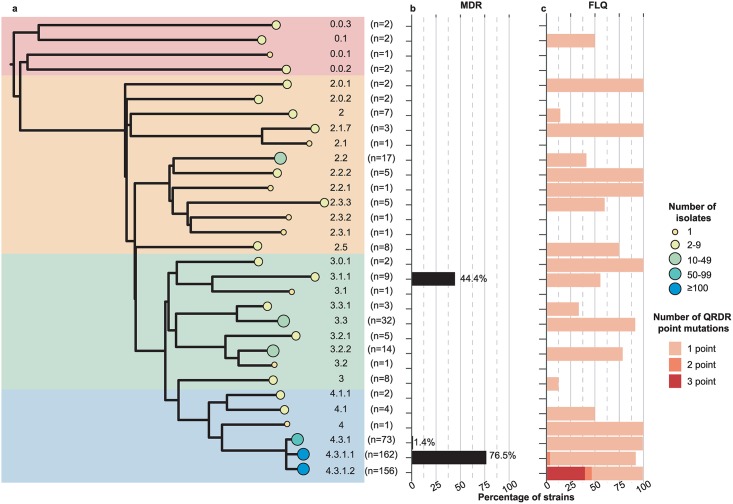
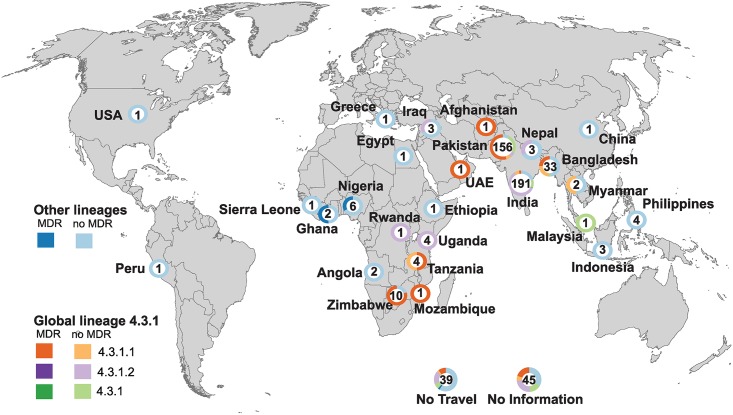
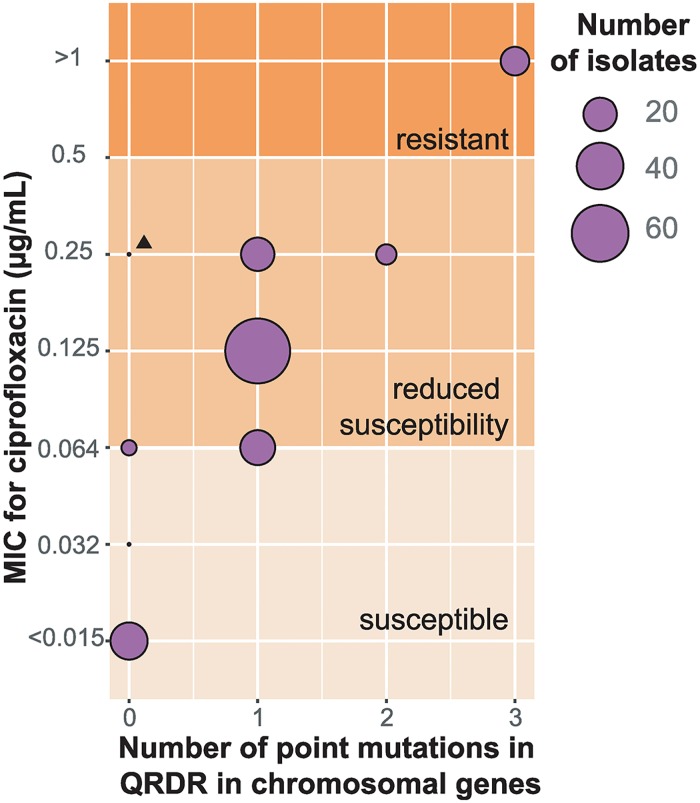
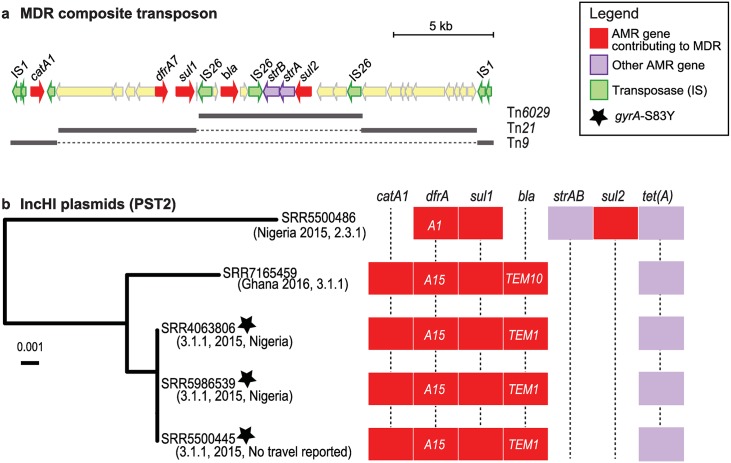
Salmonella enterica serovar Typhi (S. Typhi) is the causative agent of typhoid fever, a systemic human infection with a burden exceeding 20 million cases each year that occurs disproportionately among children in low and middle income countries. Antimicrobial therapy is the mainstay for treatment, but resistance to multiple agents is common. Here we report genotypes and antimicrobial resistance (AMR) determinants detected from routine whole-genome sequencing (WGS) of 533 S. Typhi isolates referred to Public Health England between April 2014 and March 2017, 488 (92%) of which had accompanying patient travel information obtained via an enhanced surveillance questionnaire. The majority of cases involved S. Typhi 4.3.1 (H58) linked with travel to South Asia (59%). Travel to East and West Africa were associated with genotypes 4.3.1 and 3.3.1, respectively. Point mutations in the quinolone resistance determining region (QRDR), associated with reduced susceptibility to fluoroquinolones, were very common (85% of all cases) but the frequency varied significantly by region of travel: 95% in South Asia, 43% in East Africa, 27% in West Africa. QRDR triple mutants, resistant to ciprofloxacin, were restricted to 4.3.1 lineage II and associated with travel to India, accounting for 23% of cases reporting travel to the country. Overall 24% of isolates were MDR, however the frequency varied significantly by region and country of travel: 27% in West Africa, 52% in East Africa, 55% in Pakistan, 24% in Bangladesh, 3% in India. MDR determinants were plasmid-borne (IncHI1 PST2 plasmids) in S. Typhi 3.1.1 linked to West Africa, but in all other regions MDR was chromosomally integrated in 4.3.1 lineage I. We propose that routine WGS data from travel-associated cases in industrialised countries could serve as informal sentinel AMR genomic surveillance data for countries where WGS is not available or routinely performed.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
