

Speckle tracking derived reference values of myocardial deformation and impact of cardiovascular risk factors - Results from the population-based STAAB cohort study
- PMID: 31513619
- PMCID: PMC6742365
- DOI: 10.1371/journal.pone.0221888
Speckle tracking derived reference values of myocardial deformation and impact of cardiovascular risk factors - Results from the population-based STAAB cohort study
Abstract
Aims: We aimed to provide reference values for speckle-tracking derived systolic and diastolic myocardial deformation markers, and to determine their relation with age, sex, and cardiovascular risk factors.
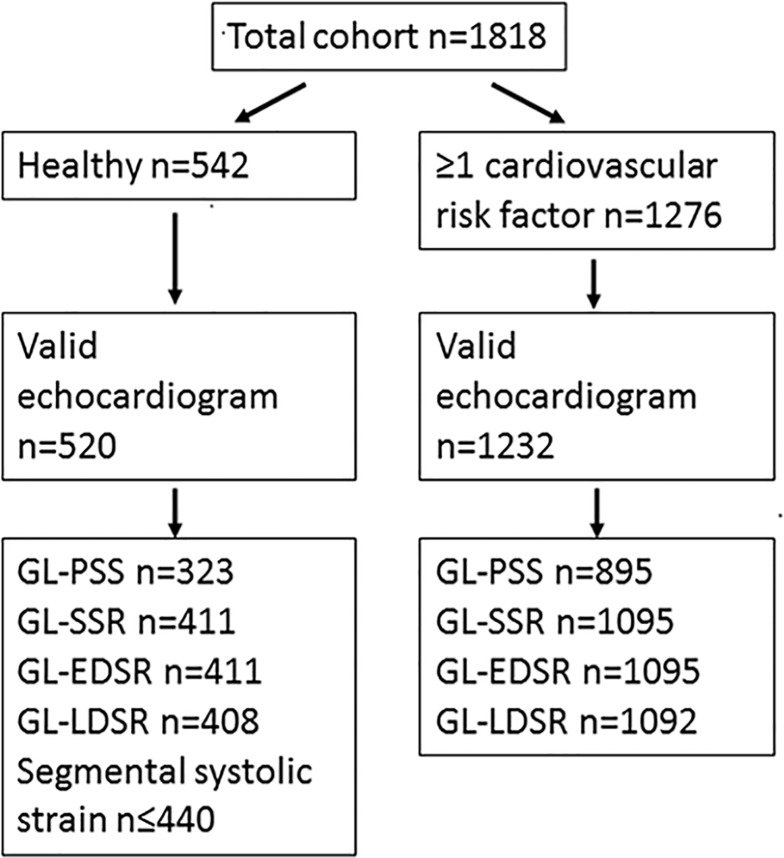
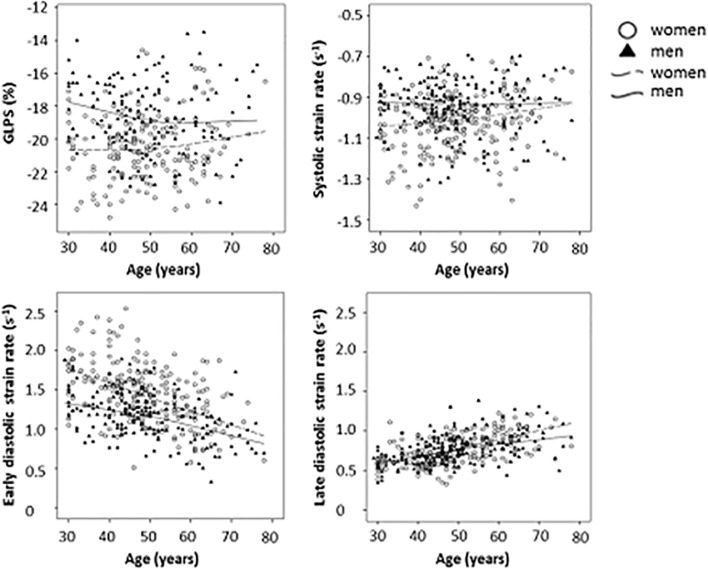
Methods and results: The Characteristics and Course of Heart Failure STAges A/B and Determinants of Progression (STAAB) cohort study recruited a representative sample of the population of Würzburg, Germany, aged 30-79 years. In a sample of 1818 participants (52% female, mean age 54±12 years) global longitudinal peak systolic strain (GL-PSS, n = 1218), systolic (GL-SSR, n = 1506), and early (GL-EDSR, n = 1506) and late diastolic strain rates (GL-LDSR, n = 1500) were derived from 2D speckle tracking analysis. From a subgroup of 323 individuals without any cardiovascular risk factor, sex- and age-specific reference values were computed. GL-PSS, GL-SSR, and GL-EDSR were associated with sex, GL-EDSR decreased and GL-LDSR increased with age. In the total sample, dyslipidemia was associated with altered GL-PSS, GL-SSR, and GL-EDSR in women but not in men, whereas obesity was associated with less favorable GL-PSS and GL-EDSR in either sex. Hypertension impacted more adversely on systolic and diastolic myocardial deformation in women compared to men (all p<0.01).
Conclusion: The female myocardium appeared more vulnerable to high blood pressure and dyslipidemia when compared to men, while obesity was associated with adverse myocardial deformation in either sex. The reference values for echocardiographic myocardial deformation provided for a non-diseased population and their here reported associations with cardiovascular risk factors will inform future observational and intervention studies regarding i) effect sizes and power calculation, ii) cross-study comparisons, and iii) categorization of myocardial deformation in specific patient groups.
Conflict of interest statement
Caroline Morbach reports a research cooperation with the University of Würzburg and Tomtec Imaging Systems funded by a research grant from the Bavarian Ministry of Economic Affairs, Regional Development and Energy, Germany, speakers honorarium from Amgen and Tomtec, a travel grant from Orion Pharma and Alnylam, and participation in Advisory and Patient Eligibility Boards sponsored by AKCEA, Alnylam, and EBR Systems outside the submitted work. Bettina Walter has nothing to disclose. Margret Breunig has nothing to disclose. Dan Liu has nothing to disclose. Theresa Tiffe has nothing to disclose. Martin Wagner has nothing to disclose. Götz Gelbrich reports a research cooperation with the University Hospital Würzburg and TomTec Imaging Systems funded by a research grant from the Bavarian Ministry of Economic Affairs, Regional Development and Energy, Germany, he receives remuneration as data safety and monitoring board member in the TIM-HF II trial (Charité Berlin), outside the submitted work. Peter Heuschmann reports grants from German Ministry of Research and Education, European Union, Charité – Universitätsmedizin Berlin, Berlin Chamber of Physicians, German Parkinson Society, University Hospital Würzburg, Robert Koch Institute, German Heart Foundation, Federal Joint Committee (G-BA) within the Innovationfond, University Hospital Heidelberg (within RASUNOA-prime; RASUNOA-prime is supported by an unrestricted research grant to the University Hospital Heidelberg from Bayer, BMS, Boehringer-Ingelheim, Daiichi Sankyo), grants from Charité – Universitätsmedizin Berlin (within Mondafis; Mondafis is supported by an unrestricted research grant to the Charité from Bayer), from University Göttingen (within FIND-AF randomized; FIND-AF randomized is supported by an unrestricted research grant to the University Göttingen from Boehringer-Ingelheim), outside the submitted work. Stefan Störk reports research grants from the German Ministry of Education and Research, European Union, University Hospital Würzburg; participation in Data Safety Monitoring and Event Adjudication and Scientific Advisory Boards in studies sponsored by Bayer, Boston Scientific; principal investigator in trials (co-) sponsored by Boehringer, Novartis, Bayer; speaker honoraria by Boehringer, Servier, Novartis, Astra-Zeneca, Pfizer, Bayer, ThermoFisher Scientific, Amgen, Alnylam, outside the submitted work. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Perk G, Tunick PA and Kronzon I. Non-Doppler two-dimensional strain imaging by echocardiography—from technical considerations to clinical applications. J Am Soc Echocardiogr. 2007;20:234–43. - PubMed
-
- Mizuguchi Y, Oishi Y, Miyoshi H, Iuchi A, Nagase N and Oki T. The functional role of longitudinal, circumferential, and radial myocardial deformation for regulating the early impairment of left ventricular contraction and relaxation in patients with cardiovascular risk factors: a study with two-dimensional strain imaging. J Am Soc Echocardiogr. 2008;21:1138–44. 10.1016/j.echo.2008.07.016 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
