

No Effect of Interstimulus Interval on Acoustic Reflex Thresholds
- PMID: 31516095
- PMCID: PMC6852360
- DOI: 10.1177/2331216519874165
No Effect of Interstimulus Interval on Acoustic Reflex Thresholds
Abstract
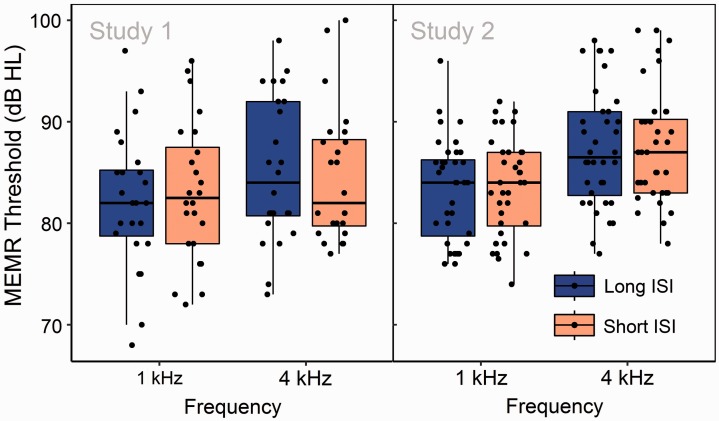
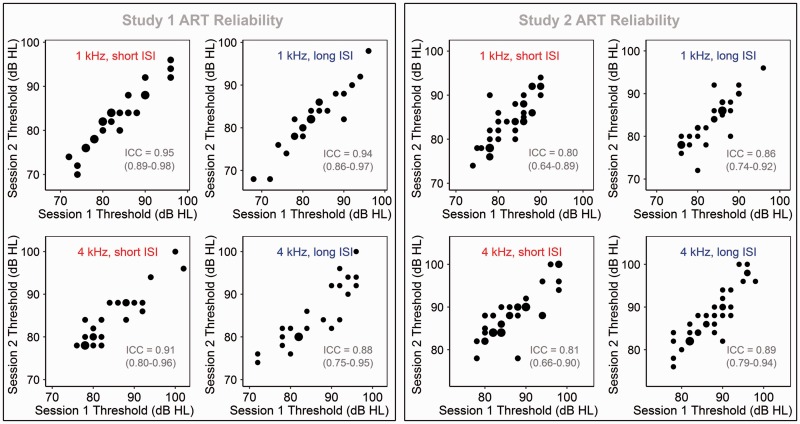
The acoustic reflex (AR), a longstanding component of the audiological test battery, has received renewed attention in the context of noise-induced cochlear synaptopathy-the destruction of synapses between inner hair cells and auditory nerve fibers. Noninvasive proxy measures of synaptopathy are widely sought, and AR thresholds (ARTs) correlate closely with synaptic survival in rodents. However, measurement in humans at high stimulus frequencies-likely important when testing for noise-induced pathology-can be challenging; reflexes at 4 kHz are frequently absent or occur only at high stimulus levels, even in young people with clinically normal audiograms. This phenomenon may partly reflect differences across stimulus frequency in the temporal characteristics of the response; later onset of the response, earlier onset of adaptation, and higher rate of adaptation have been observed at 4 kHz than at 1 kHz. One temporal aspect of the response that has received little attention is the interstimulus interval (ISI); inadequate duration of ISI might lead to incomplete recovery of the response between successive presentations and consequent response fatigue. This research aimed to test for effects of ISI on ARTs in normally hearing young humans, measured at 1 and 4 kHz. Contrary to our hypotheses, increasing ISIs from 2.5 to 8.5 s did not reduce ART level, nor raise ART reliability. Results confirm that clinically measured ARTs-including those at 4 kHz-can exhibit excellent reliability and that relatively short (2.5 s) ISIs are adequate for the measurement of sensitive and reliable ARTs.
Keywords: acoustic reflex; auditory nerve; cochlear synaptopathy; middle-ear-muscle reflex; retrocochlear disorder.
Figures
References
-
- Borg E., Odman B. (1979) Decay and recovery of the acoustic stapedius reflex in humans. Acta Oto-Laryngologica 87(5–6): 421–428. doi:10.3109/00016487909126445. - PubMed
-
- British Society of Audiology. (2011). Pure-tone air-conduction and bone-conduction threshold audiometry with and without masking. British Society of Audiology, Reading, UK.
-
- British Standards Institution. (2005). Electroacoustics. Audiometric equipment.Instruments for the measurement of aural acoustic impedance/admittance (BS EN 60645-5).
-
- British Standards Institution. (2017). Electroacoustics. Audiometric equipment.Equipment for pure-tone and speech audiometry (BS EN 60645-1).
-
- Coles R. R., Lutman M. E., Buffin J. T. (2000) Guidelines on the diagnosis of noise-induced hearing loss for medicolegal purposes. Clinical Otolaryngology and Allied Sciences 25(4): 264–273. doi:10.1046/j.1365-2273.2000.00368.x. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
