

Clinical ACO phenotypes: Description of a heterogeneous entity
- PMID: 31516821
- PMCID: PMC6733899
- DOI: 10.1016/j.rmcr.2019.100929
Clinical ACO phenotypes: Description of a heterogeneous entity
Abstract
Background: Because ACO (Asthma-COPD-Overlap) does not fill out asthma or COPD (Chronic Obstructive Pulmonary Disease) criteria, such patients are poorly evaluated. The aim of this study was to screen asthma and COPD for an alternative diagnosis of ACO, then to determine subgroups of patients, using cluster analysis.
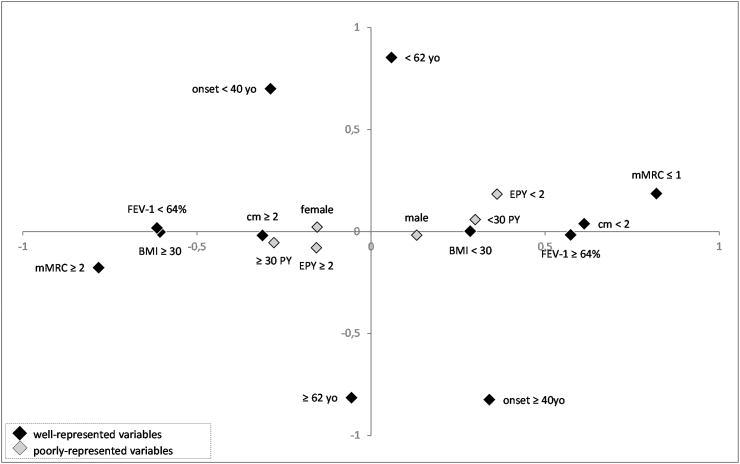
Material and methods: Using GINA-GOLD stepwise approach, asthmatics and COPD were screened for ACO. Clusterization was then performed employing Multiple Correspondent Analysis (MCA) model, encompassing 9 variables (age, symptoms onset, sex, BMI (Body Mass Index), smoking, FEV-1, dyspnea, exacerbation, comorbidity). Finally, clusters were compared to determine phenotypes.
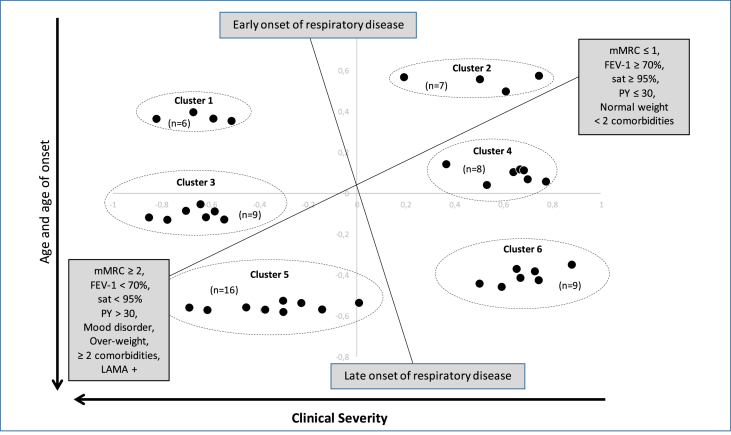
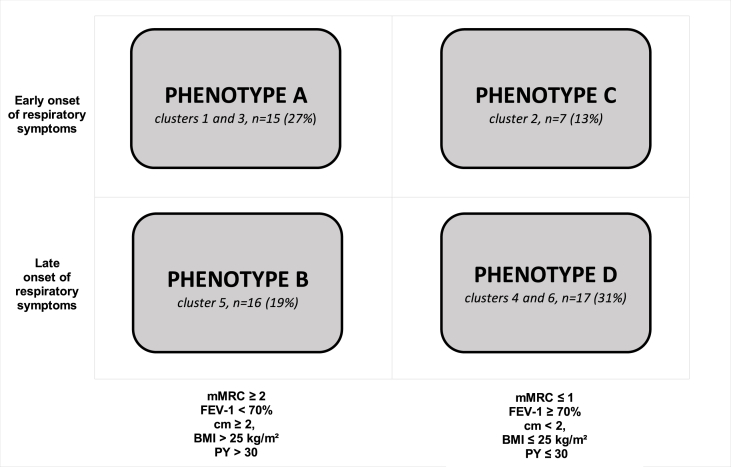
Results: MCA analysis was performed on 172 ACO subjects. To better distinguish clusters, the analysis was then focused on 55 subjects, having at least one cosine squared >0.3. Six clusters were identified, allowing the description of 4 phenotypes. Phenotype A represented overweighed heavy smokers, with an early onset and a severe disease (27% of ACO patients). Phenotype B gathered similar patients, with a late onset (29%). Patients from Phenotypes C-D were slighter smokers, presenting a moderate disease, with early and late onset respectively (respectively 13% and 31%).
Conclusions: By providing evidences for clusters within ACO, our study confirms its heterogeneity, allowing the identification of 4 phenotypes. Further prospective studies are mandatory to confirm these data, to determine both specific management requirements and prognostic value.
Keywords: ACO; Asthma; COPD; Cluster; Heterogeneity; MCA; Phenotype.
Conflict of interest statement
Dr Lainez reports grants from BOEHRINGER INGELHEIM, during the conduct of the study; Dr. Court-Fortune reports grants from BOEHRINGER INGELHEIM, during the conduct of the study; personal fees from BOEHRINGER INGELHEIM, personal fees from PFIZER, personal fees from NOVARTIS, outside the submitted work; Dr. Vercherin has nothing to disclose; Dr. Falchero has nothing to disclose; Dr. Didi has nothing to disclose; Dr Beynel has nothing to disclose; Dr. Froudarakis has nothing to disclose; Dr. Piperno reports personal fees from ASTRA ZENECA, personal fees from NOVARTIS, personal fees from VIVISOL, personal fees from ELIA MEDICAL, outside the submitted work; Dr. Devouassoux reports grants from BOEHRINGER INGELHEIM, during the conduct of the study; personal fees and non-financial support from GSK, personal fees and non-financial support fromASTRA ZENECA, personal fees and non-financial support from NOVARTIS, grants, personal fees and non-financial support from CHIESI, personal fees and other from MENARINI, outside the submitted work.
Figures
References
-
- Afrite A., Allonier C., Com-Ruelle L., Le Guen N. IRDS Publications; 2011. L’asthme en France en 2006 : prévalence, contrôle et déterminants; p. rap1820.
-
- Lister W.A., Asthma Chronic bronchitis and emphysema. Lancet. 1955;269:733–737. - PubMed
-
- Guerra S. Overlap of asthma and chronic obstructive pulmonary disease. Curr. Opin. Pulm. Med. 2005 Jan;11:7–13. - PubMed
-
- Gibson P.G., Simpson J.L. The overlap syndrome of asthma and COPD: what are its features and how important is it? Thorax. 2009;64:728–735. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
