

High serum neurofilament light chain normalizes after hematopoietic stem cell transplantation for MS
- PMID: 31516913
- PMCID: PMC6715458
- DOI: 10.1212/NXI.0000000000000598
High serum neurofilament light chain normalizes after hematopoietic stem cell transplantation for MS
Abstract
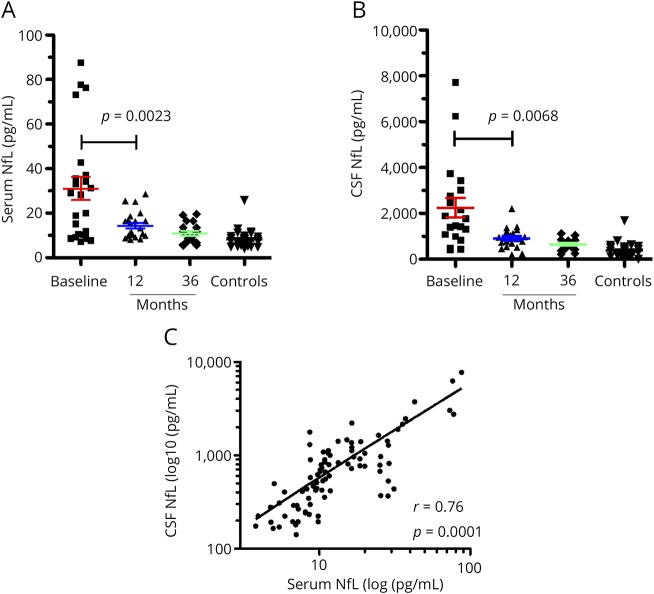
Objective: To evaluate neurofilament light chain (NfL) levels in serum and CSF of patients with aggressive MS pre- and post-treatment with immunoablation followed by autologous hematopoietic stem cell transplantation (IAHSCT) and examine associations with clinical and MRI outcomes.
Methods: Paired serum and CSF in addition to MRI and clinical measures were collected on 23 patients with MS at baseline and 1 and 3 years post-IAHSCT. An additional 33 sera and CSF pairs were taken from noninflammatory neurologic controls. NfL levels were quantitated using the Simoa platform (Quanterix).
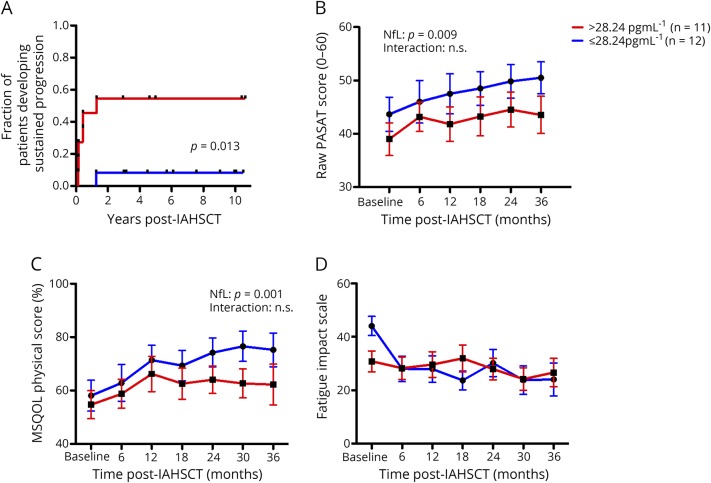
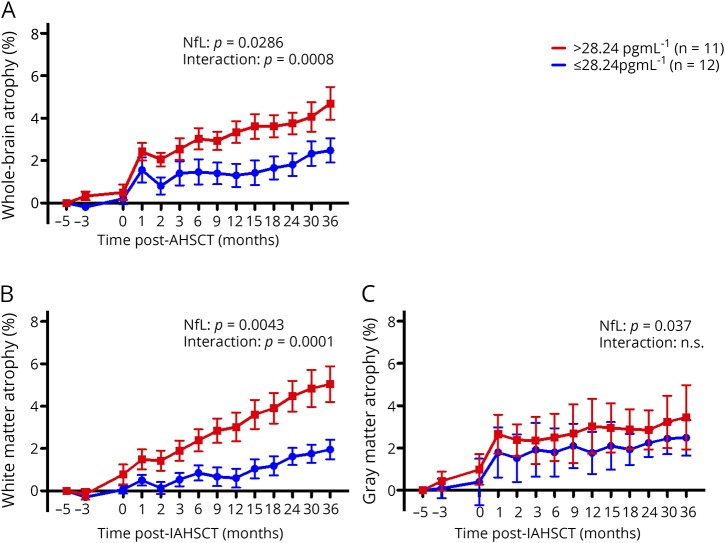
Results: Baseline MS NfL levels were significantly elevated relative to controls in serum (p = 0.001) and CSF (p = 0.001). Following IAHSCT, high pretreatment NfL levels significantly reduced in serum (p = 0.0023) and CSF (p = 0.0068) and were not significantly different from controls. Serum and CSF NfL levels highly correlated (r = 0.81, p < 0.0001). Baseline NfL levels were associated with worse pretreatment disease measures (Expanded Disability Status Scale [EDSS], relapses, MRI lesions, and MR spectroscopy (MRS) N-acetylaspartate/creatine). Elevated baseline NfL levels were associated with persistently worse indices of disease burden post-IAHSCT (sustained EDSS progression, cognition, quality of life, T1 and T2 lesion volumes, MRS, and brain atrophy).
Conclusion: These data substantiate that serum and CSF NfL levels reflect disease severity and treatment response in patients with MS and may therefore be a useful biomarker. Baseline serum levels associated with markers of pretreatment disease severity and post-treatment outcomes.
Classification of evidence: This study provides Class II evidence that for patients with aggressive MS, serum NfL levels are associated with disease severity.
Figures


Comment in
-
Blood neurofilament light chain at the doorstep of clinical application.Neurol Neuroimmunol Neuroinflamm. 2019 Aug 8;6(5):e599. doi: 10.1212/NXI.0000000000000599. eCollection 2019 Sep. Neurol Neuroimmunol Neuroinflamm. 2019. PMID: 31516914 Free PMC article. No abstract available.
References
-
- Freedman MS. Induction vs. escalation of therapy for relapsing multiple sclerosis: the evidence. Neurol Sci 2008;29:250–252. - PubMed
-
- Wattjes MP, Steenwijk MD, Stangel M. MRI in the diagnosis and monitoring of multiple sclerosis: an update. Clin Neuroradiol 2015;25:157–165. - PubMed
-
- Rovira Á, Wattjes MP, Tintoré M, et al. . Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis—clinical implementation in the diagnostic process. Nat Rev Neurol 2015;11:471–482. - PubMed
-
- Kearney H, Miller DH, Ciccarelli O. Spinal cord MRI in multiple sclerosis-diagnostic, prognostic and clinical value. Nat Rev Neurol 2015;11:327–338. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials