

Hyperkalemia in Real-World Patients Under Continuous Medical Care in Japan
- PMID: 31517144
- PMCID: PMC6734103
- DOI: 10.1016/j.ekir.2019.05.018
Hyperkalemia in Real-World Patients Under Continuous Medical Care in Japan
Abstract
Introduction: An abnormal serum potassium (S-K) level is an important electrolyte disturbance. However, its relation to clinical outcomes in real-world patients, particularly hyperkalemia burden, is not extensively studied.
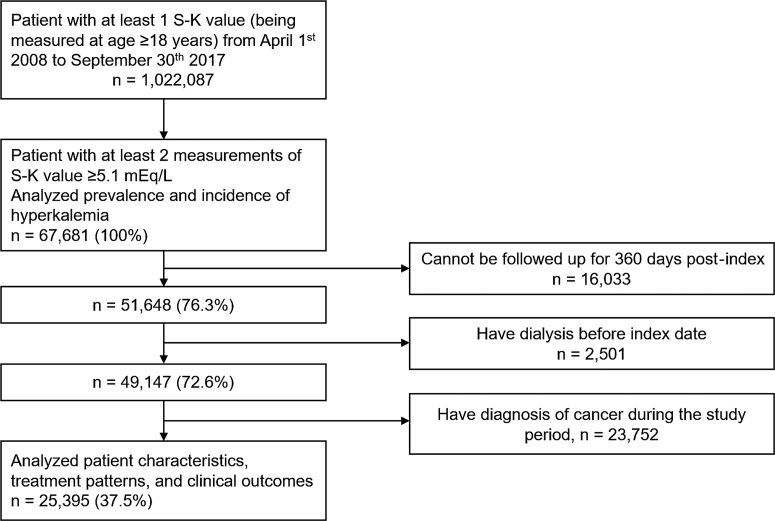
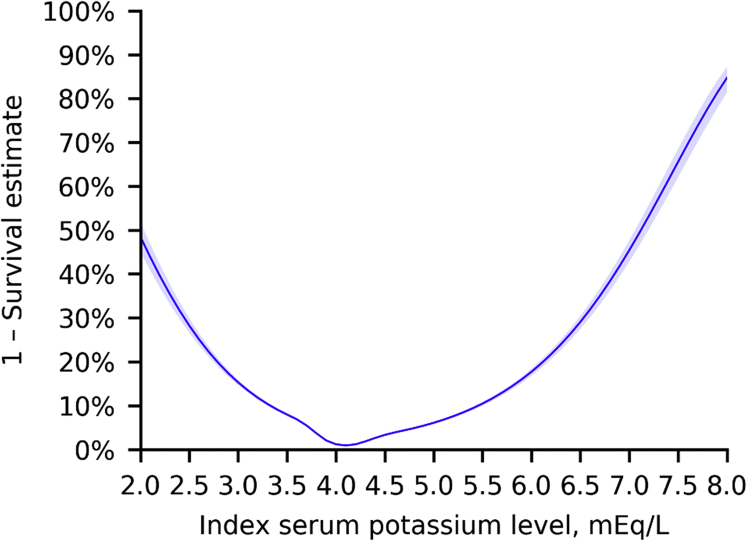
Methods: An observational retrospective cohort study using a Japanese hospital claims database was done (April 2008-September 2017; N = 1,022,087). Associations between index S-K level and 3-year survival were modeled using cubic spline regression. Cox regression model was applied to estimate the time to death according to different S-K levels. Prevalence, patient characteristics, treatment patterns, and management of patients with hyperkalemia from first episode were assessed.
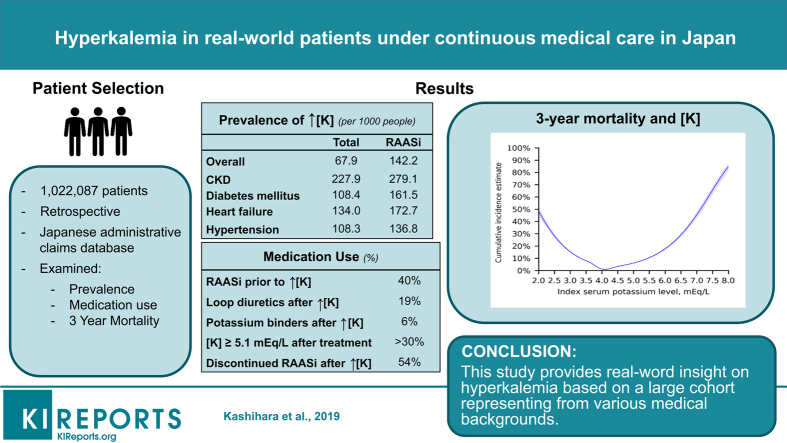
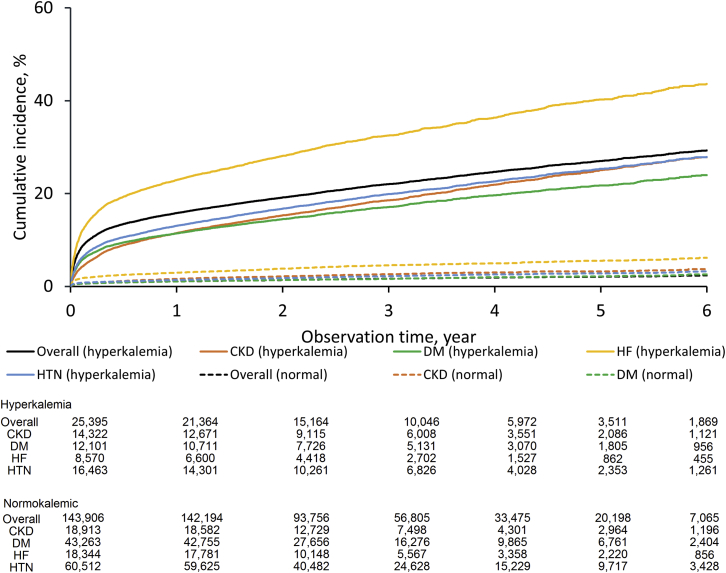
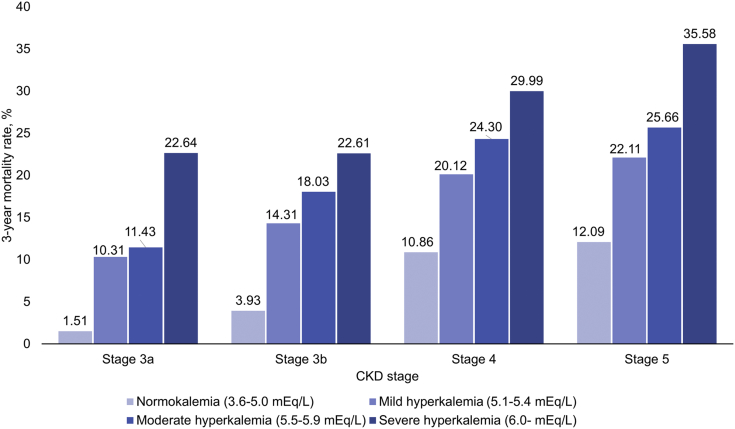
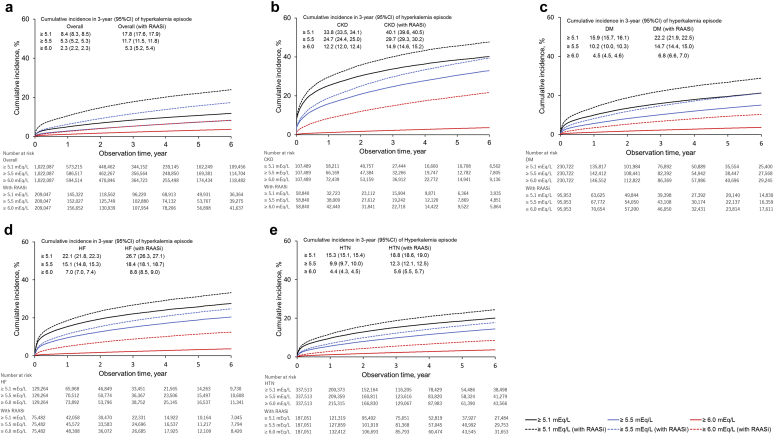
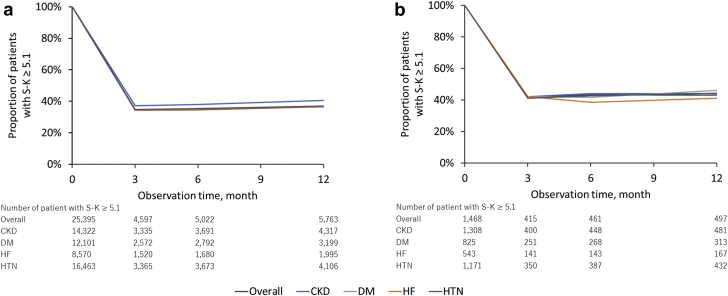
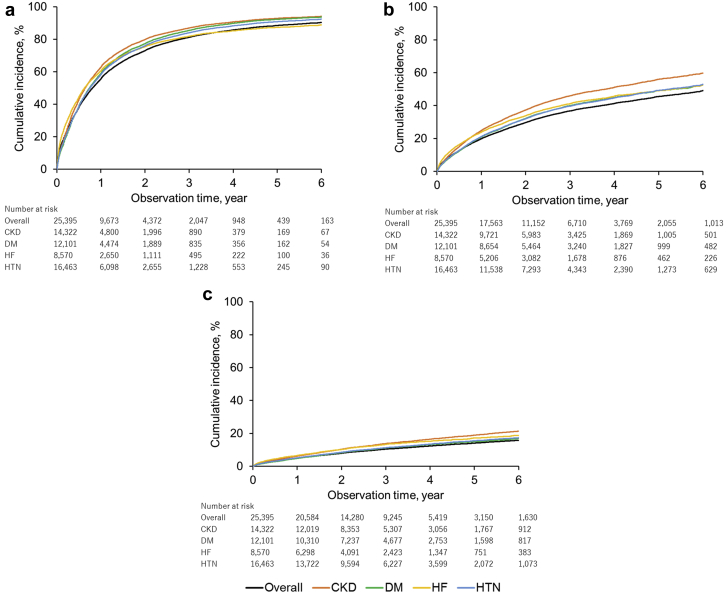
Results: Hyperkalemia prevalence was 67.9 (95% confidence interval [CI]: 67.1-68.8) per 1000 and increased in patients with chronic kidney disease (CKD) (227.9; 95% CI: 224.3-231.5), heart failure (134.0; 95% CI: 131.2-136.8), and renin-angiotensin-aldosterone system inhibitor (RAASi) use (142.2; 95% CI: 139.6-144.7). U-shaped associations between S-K level and 3-year survival were observed with nadir 4.0 mEq/l. The risk of death was increased at S-K 5.1-5.4 mEq with hazard ratio of 7.6 (95% CI: 7.2-8.0). The 3-year mortality rate in patients with CKD stages 3a, 3b, 4, and 5 with normokalemia were 1.51%, 3.93%, 10.86%, and 12.09%, whereas that in patients with CKD stage 3a at S-K 5.1-5.4, 5.5-5.9, and ≥6.0 mEq/l increased to 10.31%, 11.43%, and 22.64%, respectively. Despite treatment with loop diuretics (18.5%) and potassium binders (5.8%), >30% of patients had persistently high S-K (≥5.1 mEq/l).
Conclusion: This study provides real-world insight on hyperkalemia based on a large number of patients with various medical backgrounds.
Keywords: chronic kidney disease; congestive heart failure; hyperkalemia; renin angiotensin system; renin-angiotensin-aldosterone inhibitor.
Figures
References
-
- Palmer B.F. Managing hyperkalemia caused by inhibitors of the renin–angiotensin–aldosterone system. N Engl J Med. 2004;351:585–592. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
